INTRODUCTION
Acute coronary syndrome (ACS), which is one of the leading causes of disability, is associated with various psychiatric sequelae, such as depression and anxiety [1]. Suicidal behaviors are also common among ACS patients, and are associated with poor outcomes [2]. Suicidal ideation (SI) is a prerequisite for suicidal behaviors, including non-fatal and fatal suicidal attempts, but could also be a treatment target [3]. Identifying potential determinants of SI is thus important.
Stressful life events are major contributors to suicidal behaviors [4], although not all stressors are related to suicidal behaviors [5]. A biological component may link stressful life events with suicidal behaviors [6]. Cortisol is a widely studied effector hormone in the hypothalamus-pituitary-adrenal (HPA) axis [7]. Ghrelin, a hormone mainly produced and secreted by the stomach, penetrates the blood-brain barrier and exerts pleiotropic effects in the central nervous system [8]. Ghrelin levels are increased in animal models of depression, which has been interpreted as a stress response [9] exerted through the modulation of HPA axis activity [8]. In human studies, ghrelin levels were higher in suicide attempters than healthy controls [10,11]. However, in ACS patients, who are vulnerable to suicidal behaviors, the roles of stressful life events and ghrelin in suicidal behaviors are not well understood.
Based on existing evidence of associations of ghrelin with stress and suicidal behaviors, we hypothesized that ghrelin modulates relationships between life stressors and suicidal behaviors in ACS patients as with previous studies investigating mediating effects [12,13]. Using data from a prospective Korean cohort study, we investigated associations of life stressors with acute-phase serum ghrelin levels in ACS patients with SI, in both the acute and chronic phases, and then evaluated potential modulatory effects of serum ghrelin on associations between life stressors and SI.
METHODS
Study design and participants
Our analysis forms part a larger naturalistic, prospective study investigating the psychological sequelae of ACS [14]. Recently diagnosed ACS (ST-segment elevation myocardial infarction (MI), non-ST-segment elevation MI and unstable angina) patients seen in the Department of Cardiology of Chonnam National University Hospital, Gwangju, South Korea were recruited to the parent study in the period 2006-2012 (Supplementary Material in the online-only Data Supplement). Assessments were made within 2 weeks of hospitalization (baseline), and at 1 year thereafter (outpatient follow-up), to investigate the sequalae of ACS in both the acute and chronic phases. Life stressors and serum ghrelin levels were analyzed at baseline, while SI was evaluated in both phases. The study was approved by the Institutional Review Board of Chonnam National University Hospital. All participants provided informed consent (IRB No. 06-026).
Life stressors
Using the List of Threatening Events Questionnaire [15], nine life stressors were evaluated during the 3-month period preceding ACS diagnosis: serious illness of self, serious illness of a close relative, bereavement of a close family member, bereavement of another relative or close friend, marital separation, end of a relationship, problem or disagreement with a close friend or relative, severe economic problems, and theft or loss. The scores for each stressor were summed. Due to the skewed distribution of the data, two life stressor categories were used (absent and present).
Serum ghrelin
Participants were instructed to fast overnight before blood sampling, and to sit quietly for 25-45 min before the blood samples were drawn. Serum ghrelin levels were measured at the Global Clinical Central Lab (Yongin, Korea) using a ghrelin radioimmunoassay kit (EMD Millipore, Billerica, MA, USA). As no clear cutoffs for abnormal serum ghrelin levels have been established, the participants were divided into higher and lower ghrelin groups (median split).
Suicidal ideation
The presence of SI was identified using the ŌĆ£suicidal thoughtsŌĆØ item of the Montgomery-Asberg Depression Rating Scale (MADRS-ST) [16], which was administered by two research nurses blinding to the Mini International Neuropsychiatric Interview (MINI) results and trained and supervised by the project psychiatrist. The MADRS has been standardized in Korean [17]. This item assesses the extent to which life is perceived as not worth living, and the existence of plans for suicide; scores range between 0 (satisfied with life) and 6 (explicit plans for suicide). In this study, SI was considered present when the score on this item was Ōēź2 (and where a score of 2 corresponds to fleeting suicidal thoughts), as in previous studies [18,19].
Baseline covariates
The following sociodemographic data were collected: age, sex, duration of education, living status (living alone or cohabiting), housing status (owned or rented), and current occupation (employed or unemployed). We also obtained data on personal and family history of depression, as well as current clinical depression. The current clinical depression were determined by a psychiatrist, applying these criteria using the MINI [20], a structured diagnostic psychiatric interview for Diagnostic and Statistical Manual of Mental Disorders, 4th edition [21]. Vascular risk factors of interest included personal and family history of ACS or stroke, diagnosis of hypertension or diabetes mellitus, hypercholesterolemia (fasting serum total cholesterol level >200 mg/dL), obesity (body mass index >25 kg/m2), and current smoking status. Finally, to determine the severity of ACS, we obtained the Killip classification [22], left ventricular ejection fraction (based on echocardiography), and serum levels of the cardiac biomarkers troponin I and creatine kinase-MB.
Statistical analysis
Potential covariates were analyzed according to the presence of SI, at baseline and follow-up, using t-tests and Žć2 tests (as appropriate). Variables significantly associated with SI (p< 0.05), and those considered potentially to have an effect on suicidal behaviors [3,23], were included in subsequent adjusted analyses; collinearity was also considered. Correlations between life stressors and serum ghrelin levels were estimated by SpearmanŌĆÖs rho. The associations of life stressors (absent vs. present) and serum ghrelin (higher vs. lower) with SI, at both baseline and follow-up, were analyzed using logistic regression models before and after adjusting for covariates. Mediating effects of serum ghrelin on associations between life stressors and SI were tested for using multinomial logistic regression (adjusted model). All statistical tests were two-sided and p<0.05 was considered significant. The analyses were performed using SPSS software (ver. 27.0; IBM Corp., Armonk, NY, USA).
RESULTS
Recruitment and descriptive data
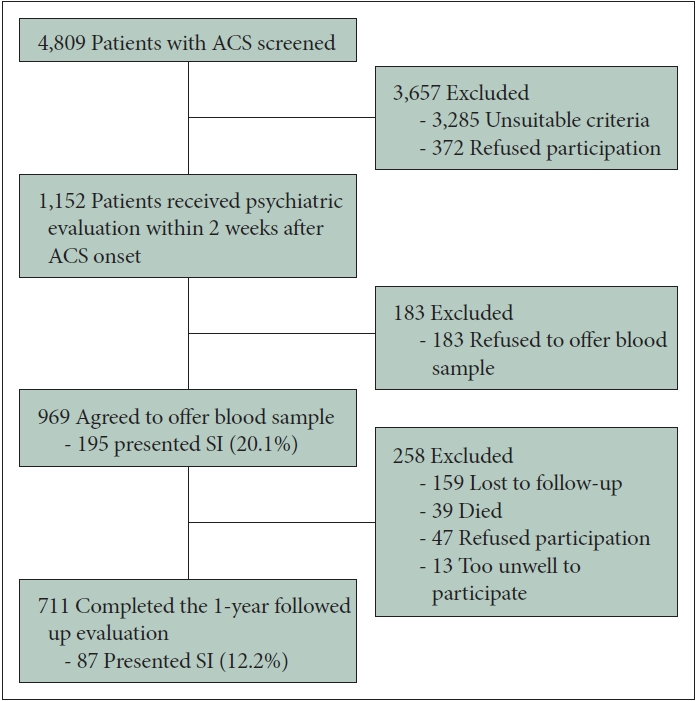
The recruitment process and prevalence of SI, at both baseline and follow-up, are summarized in Figure 1. In total, 969 ACS patients who met the eligibility criteria and agreed to provide a blood sample were included in the baseline sample. Of these patients, 711 (73%) were re-evaluated at the 1-year follow-up.
SI was present in 195 (20%) and 87 (12%) ACS patients at baseline and follow-up, respectively; the baseline characteristics of these two groups are summarized in Supplementary Table 1 (in the online-only Data Supplement). SI at baseline was significantly associated with female sex, lower education level, rented housing, current unemployment, previous and current depression, and higher troponin I levels. SI at followup was significantly associated with female sex, current unemployment, family history of depression and ACS, current depression, and diabetes mellitus. Based on the findings of this and previous studies [3,23], and on the collinearity seen among our variables, the following nine covariates were selected for subsequent adjusted analyses: sex, education, housing status, employment status, previous and family history of depression, clinical depression status, family history of ACS, and serum troponin I level.
Associations of life stressors and serum ghrelin levels with SI
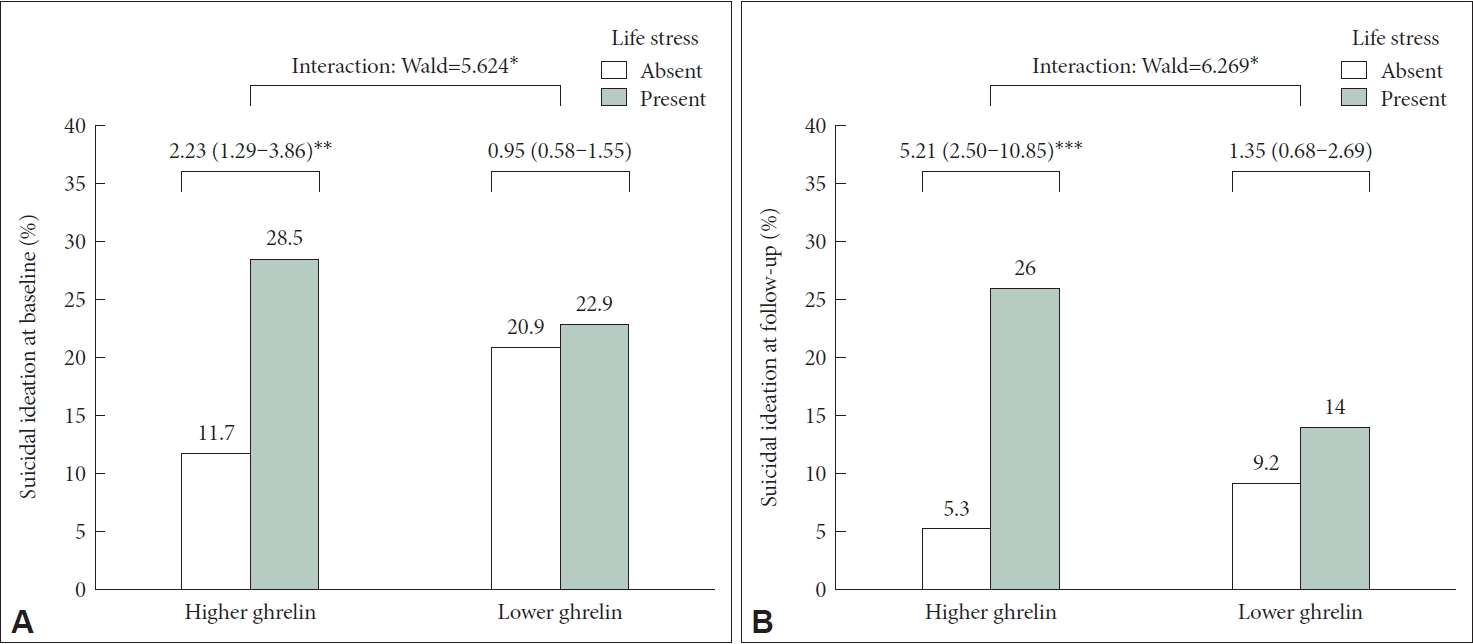
Serum ghrelin levels were positively correlated with life stressors (SpearmanŌĆÖs Žü=0.072, p=0.045). Associations of life stressors and serum ghrelin levels with SI are described in Table 1. The presence of life stressors was significantly associated with SI, at both baseline and follow-up, before and after adjustment for covariates; however, serum ghrelin levels showed no such associations. The mediating effect of serum ghrelin on associations between life stressors and SI is shown in Figure 2. Associations between life stressors and SI were significant in the higher but not in the lower serum ghrelin group; significant interaction effects were also seen after adjustment.
DISCUSSION
In this longitudinal study of ACS patients, life stressors were significantly associated with SI at baseline and follow-up. Although not associated with SI, high (but not low) serum ghrelin mediated associations of life stressors with SI; significant interaction effects were also seen after adjustment for covariates.
Life stressors are associated with suicidal behaviors in various populations, including depressive patients [4]; our findings confirmed the well-known association between these factors in both the acute and chronic phases of ACS. Previous studies reported higher serum ghrelin levels in suicide attempters than controls [10,11], but we found no such association; differences in study populations (general population vs. ACS patients) and definitions of suicidality (suicide attempt vs. SI) might account for this discrepancy.
We found that serum ghrelin levels mediated the relationships of life stressors with SI. It can be explained that there may be the relationship between the association between serum ghrelin levels and life stressors as well as between serum ghrelin levels and SI. In this study, serum ghrelin levels were significantly and positively correlated with life stressors in line with the known previous associations of ghrelin with stress response [8,9]. Moreover, given that higher serum ghrelin levels are associated with suicide attempts [10,11], it is intuitive that life stressors accompanied by high ghrelin levels may exacerbate suicidality; individuals with lower serum ghrelin levels might be less impacted by life stressors.
Regarding the limitations of this study, no data on suicide attempts or completion were obtained. However, most clinical studies of ACS also used SI as the main outcome measure, because suicidal behavior is relatively rare [19,23,24]. Also, SI was identified using a single item of the MADRS rather than using a specific psychometric instrument measuring SI. Though this method was used in previous studies [18,19], this limitation should be considered to interpret our findings. Furthermore, patients were enrolled from a single hospital, which may limit the generalizability of our findings. However, in terms of reliability (i.e., consistency among evaluations), this could also be a strength of the study. Finally, total ghrelin (rather than des-acyl ghrelin, i.e., the biologically active form that binds to the GHSR-1a) was measured, which may not fully reflect the biological activity of ghrelin. Regarding the strengths of our study, all eligible patients with recently diagnosed ACS were recruited consecutively, which increased the homogeneity of the sample. Furthermore, the patients were evaluated at similar time points (within 2 weeks of diagnosis and 1 year thereafter). Finally, we believe that this is the first study to report a mediating role of serum ghrelin in associations between life stressors and suicidality.
In conclusion, our findings provide insight into the pathogenic effects of stressors on suicidality, suggesting a mediating role of ghrelin. Regarding the clinical implications, predictions of suicidality could be improved by evaluating life stressors and serum ghrelin levels in the acute phase of ACS. It is particularly important for cardiovascular clinics to carry out such evaluations, since evaluating suicidality is challenging for untrained clinicians. Our study represents an important first step toward fully elucidating the mediating role of ghrelin in associations between life stressors and suicidality. Multicenter studies in other settings are needed to validate our findings.