INTRODUCTION
The mental health of young women is an important issue that requires psychiatric attentions. Young women at reproductive age can experience special life events such as pregnancy or childbirth. Pregnancy or childbirth is a positive and pleasant experience [1], but it could be a great burden and might induce anxiety and fear [2]. During pregnancy, women suffer from anticipating the pain of vaginal delivery and worry about sudden emergent situation requiring operation and worsening of the baby health state [2-5]. In addition, pregnant women experience an excessive weight increase and cutaneous skin change [6,7]. Physical or psychosocial changes after delivery can cause a lot of stress and difficulties in adaptation [7,8]. Many women during the postpartum undergo the feeling of decreased women attractiveness or beauty [9]. Also, women have difficulties in coping with a new baby and parenting or caring infancy [10]. Pregnancy and childbirth can change life greatly and cause stress for young women.
Depression and anxiety are common manifestations during pregnancy or after childbirth. The point prevalence of major depression during pregnancy was estimated as 3.1%-4.9% and either of major and minor depression was 8.5%-11.0% [11]. The estimated prevalence of anxiety was 35% in the third trimester of pregnancy [12]. Meanwhile, in a population-based sample of 4,451 postpartum women, 35% reported postpartum depressive symptoms and 18.0% of depressive women reported postpartum anxiety symptoms [13]. In a cohort of women within the first days after childbirth, 40.4% showed high anxiety [14]. In a community-based sample of postpartum women, the point prevalence of depression and anxiety at 14 weeks was 23.3% and 8.7%, respectively. Additionally, the point prevalence of depression and anxiety at 30 weeks was 18.7% and 16.8%, respectively [15]. A population-based survey of Australian women found that 17.4% reported depression and 12.7% reported anxiety at six months postpartum. This survey revealed that comorbid depression and anxiety was 8.1% [16]. Although the prevalence or incidence varies depending on the methods of study, the overall frequency of depression and anxiety was common.
Depression or anxiety that occurred during the peripartum period affects women’s health and childrearing. Untreated depression was associated with preterm birth, small for gestational age, stillbirth, low birth weight, and maternal morbidity [17]. Postpartum anxiety and depression have a negative influence on quality of life [18,19]. In addition, anxiety and depression during the postpartum period cause difficulties in caring infant or have a significant impact on the child’s mental health [18,20]. In severe cases, women with postpartum psychotic depression can lead to suicide and filicide [21]. The depression or anxiety during pregnancy could be a risk factor for adverse outcomes for mother and children [12,22]. Additionally, the mental health before pregnancy was likely to be a risk factor of depression or anxiety during pregnancy or postpartum [11,12,23]. Therefore, it is necessary to actively monitor the mental health in young women during pre-pregnancy for the preparation of pregnancy, as well as pregnancy and the postpartum period.
Early detection of high-risk groups on mental health in young women with pre-pregnancy, pregnancy, or the postpartum needs to be performed. The screening of the mental health in women with high-risk pregnancy or preterm labor is primarily important [24,25]. The routine screening of the mental health during pregnancy and postpartum is useful to detect high-risk of depression or anxiety [26-28]. Furthermore, considering that the mental states before pregnancy might be associated with depression or anxiety during pregnancy or the postpartum period, the screening of the mental health needs to be extended into young women expecting pregnancy and childbirth. Meanwhile, most of studies detect high-risk groups by applying a valid cutoff score on a single questionnaire. Recently, an integrated approach through cluster analysis based on multiple characteristics has been tried [29,30]. The cluster analysis could classify the high-risk group considering multiple variables on the mental health states. When using the cluster analysis, it could be classified into the same cluster if it shows values close to the cutoff even below the cutoff. It could be a useful classification for monitoring groups that are likely to develop into high-risk groups, as well as high-risk groups. Therefore, this study aimed to examine and classify the mental health in a community sample of young women with pre-pregnancy, pregnancy, or postpartum using cluster analysis.
METHODS
Subjects
A total of 293 subjects were participated in this study from January 1, 2022 to June 30, 2022. Inclusion criteria were 1) young women over age 18 years, 2) young women expecting pregnancy, being pregnant or being during postpartum period, and 3) people who consent to this study. Exclusion criteria were 1) women who are unable to conceive or are in menopause, 2) those who have an intellectual disability that makes it difficult to answer questionnaires, and 3) illiterate people. This study was approved by Institutional Review Board at Pusan National University Hospital (PNUH IRB: No 2203-033-112).
Design
This study was cross-sectionally performed to evaluate and classify the mental health of young women during pre-pregnancy, pregnancy, or the postpartum period. The pre-pregnancy period in this study was considered for women who are over age 18 years and before menopause, as well as who can be conceived. Demographic and basic clinical variables such as age, current pregnant state, experience of delivery, and premenstrual syndrome were assessed. Clinical variables on the mental health such as depression, anxiety, stress perception, and quality of life were evaluated by Patient Health Questionnaire-9 (PHQ-9), Generalized Anxiety Disorder-7 (GAD-7), Perceived Stress Scale (PSS), and World Health Organization Quality of Life Scale Abbreviated Version (WHOQOL-BREF). For the subjects who already experienced a delivery or deliveries, postpartum depression was measured by Edinburgh Postnatal Depression Scale (EPDS). Demographic and clinical variables were examined by the Internet of Things-based mental health monitoring system for the young women that is a convenient evaluation system using a tablet PC.
Measurements
PHQ-9
The PHQ-9 was developed to screen the high-risk group of depression and assess the severity of depression [31]. The PHQ-9 consists of 9-item questions ranging from 0 to 27 and higher scores suggest the increase of the severity of depressive symptoms. The Korean version of the scale used in this study had acceptable reliability and validity [32].
PSS
The PSS is a self-report questionnaire to measure the level of stress perception in stressful situations [35]. It contains 10-item questions about negative perception and positive perception ranged from 0 to 40 scores and higher scores reflect more severe perceived stress. The Korean version of PSS showed acceptable psychometric properties [36].
WHOQOL-BREF
The WHOQOL-BREF is a brief version of the self-report World Health Organization Quality of Life Scale (WHOQOL) [37]. The WHOQOL-BREF consists of total 26-items to measure the subjective quality of life related to 4 subdomains (physical health, psychological health, social relationship, and living environment), ranging from 26 to 130. Higher scores demonstrate better quality of life. In this study, the total score acquired by summing of all questions reflecting the general quality of life was used without distinguishing each domain. The Korean version of WHOQOL-BREF in this study showed valid psychometric properties [38].
EPDS
The EPDS is a self-report scale to assess postpartum depression [39]. It consists 10 questions to measure depression, anxiety, and suicidal ideation for a week using a Likert scale of 0 to 3 points. The Korean version of the scale in this study showed valid psychometric properties [40]. The internal agreement of this scale was 0.85, and this scale was highly correlated with Beck Depression Inventory and Hamilton Depression Rating Scale.
Statistical analysis
The subjects in this study were classified by cluster analysis based on clinical characteristics such as depression, anxiety, stress perception, and quality of life. A hierarchical clustering was performed to determine the proper cluster number based on the elbow method and clinical relevance. Based on the cluster number by a hierarchical clustering, k-means clustering was performed. Among the groups classified by the results of cluster analysis, the clinical variables such as PHQ-9, GAD-7, PSS, WHOQOL-BREF, and EPDS were compared by analysis of variance and Bonferroni post hoc test. Categorical variables were analyzed by chi-square test. In addition, the frequency of high-risk subjects among clusters using cutoff scores of PHQ-9 (≥8 or ≥11) [41] and GAD-7 (≥5 or ≥15) [33] was compared by the chi-square test. A statistical analysis was performed using the SPSS 22.0 statistical program (IBM Corp., Armonk, NY, USA) with a significance level of p<0.05.
RESULTS
Demographic and clinical characteristics of the subjects
Demographic and clinical characteristics of the 293 subjects were shown in Table 1. The mean age of the subjects was 32.5± 5.1 years. The number of subjects who are currently pregnant state was 121 (41.3%), while 76 (25.3%) of the subject had experiences of delivery in the past. Also, 74 subjects (25.3%) experienced premenstrual syndrome. The mean PHQ-9 score was 6.7±5.9, the mean GAD-7 score was 3.9±4.4. The mean scores of PHQ-9, GAD-7, PSS, and WHOQOL-BREF were 6.7±5.9, 3.9±4.4, 28.7±4.7, and 53.1±10.0, respectively, while the mean EPDS score of the 76 subjects experienced delivery was 10.4±6.5.
Cluster analysis based on the mental health states
Using the information on the mental health states such as depression, anxiety, stress perception, and quality of life, the subjects were clustered. Based on the results of a hierarchical clustering and clinical relevance, a classification of three groups was determined to be adequate, therefore k-means clustering clustered the subjects into three groups.
Comparison of clinical characteristics among clusters based on the mental health status
As shown in Table 2, there were significant differences of the PHQ-9, GAD-7, WHOQOL-BREF, and EPDS total scores (PHQ-9, p<0.001; GAD-7, p<0.001; WHOQOL-BREF, p<0.001; EPDS, p<0.001) among three cluster groups. PHQ-9, GAD-7, and EPDS total score in cluster 2 group were significantly higher than those of cluster 3 and 1 groups (p<0.001). Total score of the PHQ-9, GAD-7, and EPDS scales in cluster 3 were also significantly higher than those of cluster 1 group (p<0.001). Meanwhile, the WHOQOL-BREF total score of cluster 2 was significantly lower than those of cluster 1 (p<0.001) and cluster 3 (p<0.001). In addition, there was significant difference of experience of premenstrual syndrome among three clusters. The cluster 2 showed the highest frequency of premenstrual syndrome experience.
Comparison of the frequency of high-risk subjects among clusters using cutoff scores of PHQ-9 and GAD-7
The frequencies of high-risk subjects among clusters using cutoff scores of PHQ-9 and GAD-7 is shown in Table 2. When adapting the PHQ-9 cutoff score equal or greater than 8 or 11, there were significant differences of the frequency of high-risk subjects among clusters (PHQ-9 cutoff score ≥8, p<0.001; PHQ-9 cutoff score ≥11, p<0.001). In case of the PHQ-9 cutoff score ≥8, the frequencies of high-risk subjects were 13.6% in cluster 1, 89.1% in cluster 2, and 43.1% in cluster 3, respectively. In case of the PHQ-9 cutoff score ≥11, the frequencies of high-risk subjects were 5.8% in cluster 1, 71.7% in cluster 2, and 22.2% in cluster 3, respectively.
When adapting the GAD-7 cutoff score equal or greater than 5 or 15, there were significant differences of the frequencies of high-risk subjects among clusters (GAD-7 cutoff score ≥5, p<0.001; GAD-7 cutoff score ≥15, p<0.001). In case of the GAD-7 cutoff score ≥5, the frequencies of high-risk subjects were 9.7% in cluster 1, 87.0% in cluster 2, and 41.7% in cluster 3, respectively. When the GAD-7 cutoff score ≥15, the frequencies of high-risk subjects were 1.0% in cluster 1, 26.1% in cluster 2, and 2.1% in cluster 3, respectively.
DISCUSSION
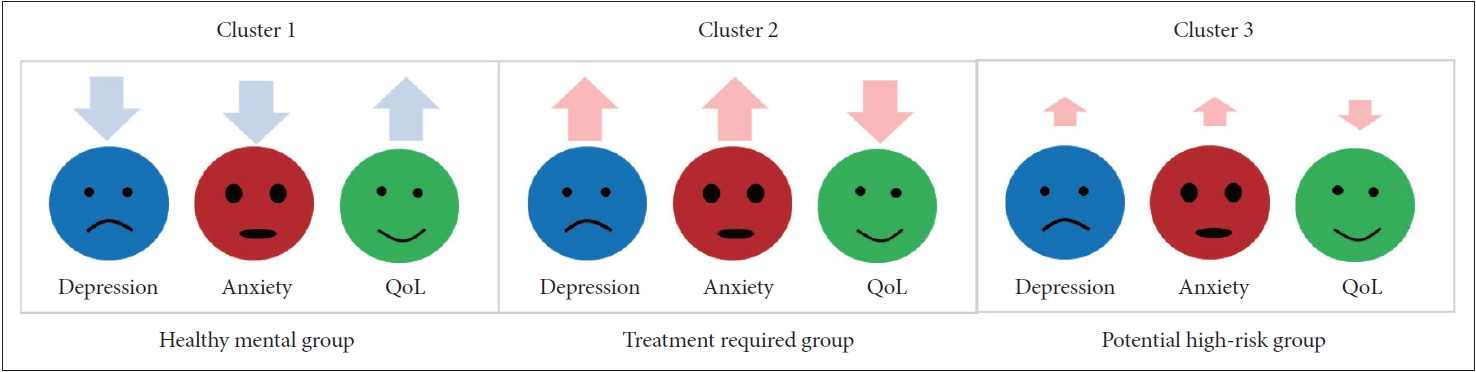
Cluster analysis based on the mental health of young women with pre-pregnancy, pregnancy, or postpartum was performed. This study showed that the mental health in young women might be classified into three clinically relevant clusters (Figure 1). Cluster 1 showed low depression, anxiety, and high quality of life that this group represented people with healthy mental states and rare experience depression and anxiety. Cluster 2 showed high depression, anxiety, and low quality of life. The PHQ-9 and GAD-7 scores of cluster 2 were above the cutoff score for screening depressive disorder and anxiety disorder. The quality of life of this cluster was significantly low. Considering the findings of previous studies [42,43], the low quality of life might be caused by depression and anxiety. Taken together, cluster 2 may comprise young women who are suffering from depressive disorder and anxiety disorder. Meanwhile, cluster 3 indicated intermediate characteristics between cluster 2 and cluster 1. Although the mean scores of PHQ-9 and GAD-7 were lower than the optimal cutoff for depressive disorder and anxiety disorder, the mean PHQ-9 and GAD-7 scores of cluster 3 were close to the cutoff score for screening depression and anxiety [33,41]. If the sensitivity was prioritized when detecting a high risk group, cluster 3 might be the potential high-risk group requiring a psychiatric evaluation in detail.
Meanwhile, there were significant differences of the EPDS scores and the frequencies of premenstrual syndrome among the clusters, similar to the severity of depression and anxiety. When compared the EPDS scores among the clusters, the score of EPDS in cluster 2 representing group in need of treatment was higher than those of cluster 3 and 1. Although the comparison on the severity of postpartum depression was only analyzed in the subjects who experienced the delivery, the results was cautiously interpreted. However, even though the proportion of experience of delivery among clusters did not show the significant difference, the severity of postpartum depression measured by the EPDS showed a significant difference among clusters. That is, the subjects in need of psychiatric treatment on depressive and anxiety disorders irrespective of the experience of the delivery had similarity to the subjects of high-risk groups of postpartum depression among women who experienced the delivery.
In addition, the frequency of premenstrual syndrome was also the highest in cluster 2. Like the severity of postpartum depression, the subjects experiencing the premenstrual syndrome had a similarity to depression and anxiety in cluster 2. These results suggest that classification using cluster analysis can be useful in classifying treatment requiring group or potential high-risk group in need of detailed monitoring. In addition, it can be seen as suggesting the need to monitor related characteristics such as depression, anxiety, quality of life, and premenstrual syndrome from the preparation stage for pregnancy in order to predict rapidly and intervene depression during pregnancy or postpartum depression. Of course, since the results of this study are classified based on the similarity of the mental health of young woman subjects in a community, it is necessary to analyze the results of previous studies according to each period in order to clearly identify causal relationships and risk factors in the community sample.
On the other hand, there was no significant difference in stress perception in cluster analysis classified based on mental health. Considering the general effect of stress on mental health, it is curious that there was no difference in stress perception among three clusters. It means that the stress level of the subjects participating in this study was high, compared to healthy population [44]. The overall levels of perceived stress of the subjects in this study was similar to patients with mood disorders [45,46]. Otherwise, it can be said that this indirectly shows the possibility that young women related to pregnancy or delivery are likely to be more stressed than other healthy groups. The results related to perceived stress in this study lead to a necessity of future study to investigate the perceived stress on young women during pre-pregnancy, pregnancy, or the postpartum period.
There are some limitations. Firstly, the number of subjects participating in this study was not sufficiently large to confirm the characteristics of three cluster groups. In the future, a largescale study needs to be conducted. Secondly, this study was performed cross-sectionally. The prospective study on the longitudinal course in three cluster groups needs to be done. Especially, if the proper management to the potential highrisk group like cluster 3 is not provided, the possibility of this group into the progression of depressive or anxiety disorder should be explored. Thirdly, this study included all of young women during pre-pregnancy, pregnancy, or the postpartum period, not divided each group according to the status of pregnancy or postpartum, although most of previous studies classified normal group and high-risk groups according to the status of pregnancy or postpartum, respectively. For this reason, these findings cannot be the prevalence or incidence of the subjects with depressive or anxiety disorders or high-risk. Instead, the results of cluster analysis revealed the global patterns on the mental health in young women with pre-pregnancy, pregnancy, or postpartum. Additionally, instead of the result of single questionnaire based on the cutoff score, the similarity among multiple variables on the mental health states was used to classify the groups. Like this study, a clustering approach that considers several variables simultaneously may be meaningful to detect or monitor the high-risk groups on the mental health in young women.
In conclusion, this study reported that the subjects were classified into three groups by cluster analysis. The results of this study suggested that young women in a community might be in the group with good mental health, high-risk group requiring active monitoring the mental health, or group in definite need of treatment. By monitoring their mental health, the groups with high-risk or requiring treatment are warranted to be explored and provided proper management for improvement of mental health and quality of life. Although the screening of single questionnaire using the cutoff score is still important, the cluster analysis considering multiple factors might be useful to classify the high-risk of the mental health. Based on the cluster analysis, the classification of mental health in the community would be a useful approach for early detection and appropriate management of mental health problem in young women. In the future, if a database system in the community is established, the classification of the mental health groups would be updated based on the collected data. The screening system using cluster analysis based on the mental health states would be useful and effective to discover and treat appropriately at the time of early symptoms. These findings in this study would be the basic evidence on feasibility of early detection using cluster analysis.