INTRODUCTION
According to the Global Burden of Disease Study, 2019, dementia was the seventh leading cause of death globally, accounting for 1.6 million deaths [1]. Individuals with any type of dementia have an average mortality risk 5.9 times higher than those without dementia [2]. However, given its phenotypic heterogeneity, with varying symptoms and disease trajectories, survival in such populations is highly variable [2,3]. Therefore, the development of prediction models for the risk of mortality among individuals with dementia is important for future planning and service provision.
Most previous studies have emphasized a single patient- or disease-specific factor in predicting mortality risk among individuals with dementia, such as age, male sex, presence of comorbidities, bone fracture, stroke, and/or nasogastric (NG) intubation [4-6]. However, the single-disease paradigm may not be adequate for individuals with dementia because they frequently have multiple chronic conditions. To date, few studies have examined multiple factors and their inter-relationship(s) in predicting mortality in patients with dementia. Furthermore, most current prediction models for mortality in patients with dementia are limited by several methodological designs that confer a higher risk for bias or diminished generalization and applicability [7]. Other concerns include underestimation of physical comorbidities [8], restricted/specific populations, and a shorter mortality prediction period (<1 year) [9]. For example, a prognostic model using claims data from the Swedish Dementia Registry (SveDem) can predict mortality risk at 3 years among patients with dementia. However, SveDem covers approximately 35% of incident dementia [10], and patients included in the SveDem are more likely to be male, younger, and healthier, thus limiting the generalizability to other populations [11]. In addition, the diagnosis of chronic medical conditions, such as diabetes mellitus, may be underdiagnosed in patients [8]. Another study provided the best validated prognostic model for predicting the risk for mortality for only 6 months, and this model applied a specific population of patients with advanced dementia from nursing homes [9].
Dementia can complicate chronic conditions and vice versa [12]. On average, patients with dementia have 2 to 8 comorbidities [13]. Previous large cohort studies involving community-dwelling individuals with dementia found that those with comorbid diabetes and heart disease, such as myocardial infarction, experienced higher mortality during the follow-up period [14,15]. Therefore, adopted robust multivariable prediction models must consider not only individual-level risk factors but also their inter-relationships with mortality, particularly in heterogenous diseases such as dementia. Latent class analysis (LCA) can be used to identify distinctive—but unmeasured—subgroups within a heterogeneous population [16]. Using LCA, it is possible to categorize dementia based on the numbers of patient- and disease-specific factors rather than a single individual risk factor in predicting mortality. The LCA approach has been used in several previous studies investigating the homeless veteran population [17], acute kidney injury [18], and type 2 diabetes [19]. To the best of our knowledge, however, no study has used LCA to predict mortality risk in patients with dementia.
To identify which multimorbidity pattern may be associated with an increased risk for mortality, we applied LCA to data from a nationally representative sample of patients with dementia. We hypothesized that there were latent classes of patients with dementia characterized by specific phenotypes and risk for mortality, which may have clinical implications for physicians with regard to early detection and intervention.
METHODS
The nationwide cohort was derived from the Taiwan National Health Research Database (NHIRD), which is audited and released by the Taiwan National Health Research Institute for Scientific Studies [20,21]. At the end of 2010, the coverage rate for the NHIRD was approximately 99.6% (23 million residents). Comprehensive information regarding insured individuals is housed in the database, including demographic information, clinical visit dates, disease diagnoses, and prescriptions. The insurance claim information of individuals is kept anonymous to maintain privacy. In the present study, using each resident’s unique personal identification number, all information was linked. The diagnostic codes used were based on the International Classification of Diseases, 9th revision, Clinical Modification (ICD-9-CM). The NHIRD has been used extensively in many Taiwanese epidemiological studies [22-24]. The study protocol was reviewed by the Institutional Review Board of the Taipei Veterans General Hospital (2018-07-016AC).
Patients ≥65 years of age diagnosed with dementia (ICD-9-CM codes 290.0-290.4, 331.0-331.2, and 294.1), confirmed by board-certified neurologists or psychiatrists at least twice based on comprehensive interviews and clinical judgement between January 1, 2002 and December 31, 2009, were included. The dementia cohort was followed until December 31, 2013 or until death (whichever occurred first). In Taiwan, a diagnosis of dementia needs to be based on the results of blood examinations (complete blood count and biochemistries, iron, thyroid hormone, vitamin B12, folate, and syphilis), psychological tests, and brain imaging. The condition of mortality was identified from the claims data or registry of catastrophic illness [25]. The mortality risk in patients with early onset dementia was not examined.
A consensus meeting with a team of neurologists and psychiatrists experienced in dementia care was convened to identify the relevant morbidity conditions. Besides, we consulted several index papers [14,26-28] addressing morbidities in patients with dementia. Morbid conditions represented the status of conditions or diseases that patients with dementia exhibited upon clinic visits or hospitalization at the time of a diagnosis of dementia. Acute clinical conditions (existing within 3 months before the first diagnosis of dementia) were also included. Finally, the following 16 morbidity conditions were included: diabetes mellitus; hypertension; dyslipidemia; coronary artery disease; congestive heart failure; myocardial infarction; cancer; stroke; bone fracture; peripheral vascular disease; chronic kidney disease; chronic obstructive pulmonary disease (COPD); upper gastrointestinal (UGI) bleeding; pulmonary infection; urinary infection; and NG intubation.
Statistical analysis
Patients with dementia were divided into six groups based on age (65-69, 70-74, 75-79, 80-84, 85-89, and ≥90 years). The 16 morbidity conditions (absence vs. presence) and sex were dichotomized. Descriptive statistics were used to describe the demographic characteristics and prevalence of each morbidity condition. The distribution of demographics and the prevalence of morbidity conditions among the different age groups were examined using analysis of variance with post hoc Bonferroni correction.
LCA was used to generate clusters of morbidity conditions among participants, which could identify a set of underlying subgroups of individuals based on the intersection of multiple observed characteristics. In practice, it is unlikely that every observed characteristic actually reflects a unique and important type of individual; therefore, it may be helpful to establish a smaller set of subgroups with specific multimorbidity patterns that may correlate with mortality. Such subgroups are unobserved and are referred to as “latent classes.” The observed categorical variables that comprised the latent classes in this analysis included sex and the 16 morbidity conditions. Age was also included as a covariate because it is strongly associated with mortality. The LCA model was fit over two, three, and four. The class with the smallest Bayesian information criterion (BIC) and Akaike information criterion (AIC) was considered to be a good fit. Participants were classified into latent classes based on the maximum predicted probability. The predicted latent classes and the risk for mortality were examined using logistic regression, with adjustment for sex, age, and the 16 morbidity conditions. In summary, LCA analysis often followed three steps: 1) to build a latent class model for a set of observed discrete variables; 2) subjects are assigned to latent classes based on their highest membership probability; and 3) using these predicted scores to assess the association between the assigned class membership and external variables via simple cross-tabulations or multinomial logistic regression analysis.
We chose 5-year mortality rate based on our previous study, which shown the mean survival time from diagnosis was 5.8 and 4.6 years for Alzheimer’s disease (AD) and non-AD dementia, respectively [2]. Data management and analysis were performed using Stata version 16 (StataCorp LLC, College Station, TX, USA) and the R-Project version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria). Differences with a two-tailed p<0.05 were considered to be statistically significant.
RESULTS
Descriptive summaries of dementia according to age group
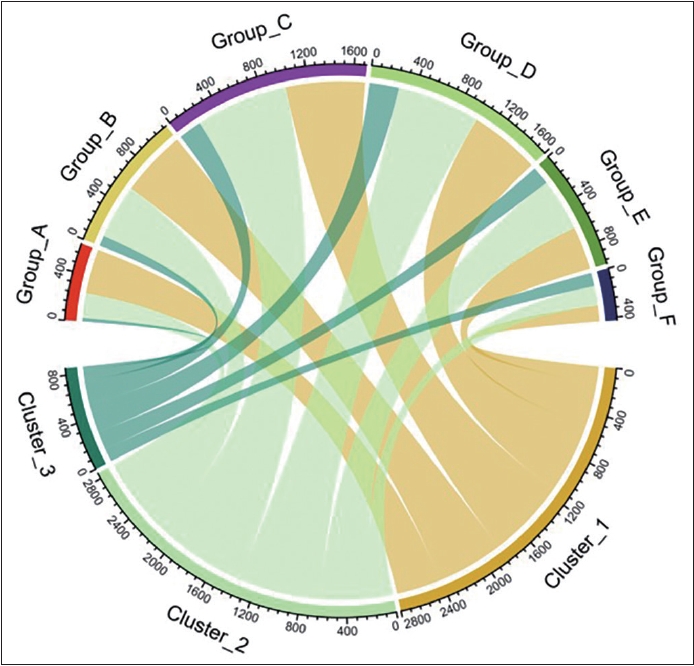
Demographic characteristics of patients with dementia for each age group are summarized in Table 1. Patients were divided into six groups according to age (in years): A, 65-69; B, 70-74; C, 75-79; D, 80-84; E, 85-89; and F, ≥90. The sample sizes in each group ranged from 426 in group F (≥90 years) to 1,701 in group C (75-79 years). Females constituted most patients across the groups, with group A (65-69 years) containing the highest proportion of female patients. The 5-year mortality rate ranged from 14.8% to 42.0%, with group F (≥90 years) exhibiting the highest mortality rate. There were significant differences in age, sex, stroke, bone fracture, medical history, and 5-year mortality across the groups. Post hoc analysis using the Bonferroni method was performed to compare baseline differences between groups.
LCAs
Based on the AIC and BIC, the three-class model was the most parsimonious with optimal clinical interpretability and class size. Because age represents the most significant risk factor for higher mortality in patients with dementia [2,29], the LCA model was adjusted for age. Individuals from each age group were equally distributed in clusters 1, 2, and 3 (Figure 1).
Because comorbid disease has been reported to be the main predictor of mortality in community-dwelling older adults with dementia [15], three clusters were defined: cluster 1, low comorbidity class (n=2,800); cluster 2, cardiometabolic multimorbidity class, defined as ≥2 cardiometabolic conditions [30] (n=2,900); and cluster 3, FRINGED class, which was characterized by FRacture, Infection, NasoGastric feeding, and bleEDing over the UGI tract (n=856).
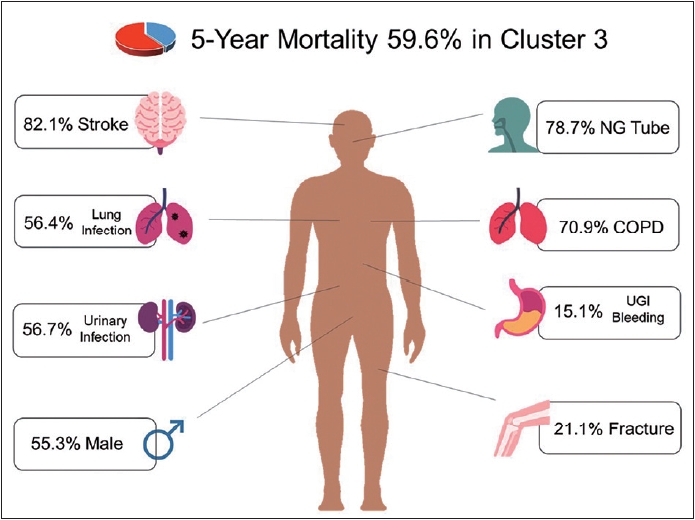
The baseline characteristics of each latent class are summarized in Table 2. There was no significant difference in age across the three clusters. Most patients were female in clusters 1 and 2, while most were male in cluster 3. Regarding stroke and bone fracture, the proportion was highest in cluster 3 (82.1% and 21.1%, respectively). The prevalence of several medical histories, including COPD, UGI bleeding, lung infection, NG intubation, and urinary infection, was lowest in patients in cluster 1. The clusters were numbered according to increased 5-year mortality risk: cluster 1 had the lowest (17.6%), whereas cluster 3 had the highest (59.6%). Important characteristics of the patients comprising cluster 3 are shown in Figure 2. Several different types of comorbidities were observed in cluster 3, in which stroke (82.1%), NG intubation (78.7%), and COPD (70.9%) were most common.
Predictability of 5-year mortality of latent class and other variables
The comorbidity and characteristic clusters among patients with dementia from the LCA are shown in Supplementary Figure 1 (in the online-only Data Supplement). Associations of 5-year mortality with the latent classes are summarized in Table 2. Cluster 1 was set as the reference group for analysis. Patients in clusters 3 (odds ratio [OR]=9.828 [95% confidence interval, CI=6.708-14.401]; p<0.001) and clusters 2 (OR=1.582 [95% CI=1.281-1.953]; p<0.001) had the highest and secondhighest 5-year mortality rate, respectively, compared with those in cluster 1 during the follow-up period (Table 3). Regarding different age groups, age-dependent risk for mortality was found in groups C to F (group C, OR=1.660 [95% CI=1.285-2.146]; group D, OR=2.067 [95% CI=1.601-2.668]; group E, OR=2.139 [95% CI=1.630-2.806]; and group F, OR=2.829 [95% CI=2.066-3.874]). Patients in group C to group F exhibited a higher 5-year mortality rate compared with those in group A and there was no difference regarding 5-year mortality rate between Group A and B. Significant risk factors for higher 5-year mortality identified in this study included male sex (OR=1.705 [95% CI=1.510-1.927]), cancer (OR=1.709 [95% CI=1.491-1.959]), diabetes (OR=1.194 [95% CI=1.053-1.352]), chronic kidney disease (OR=1.632 [95% CI=1.370-1.943]), and congestive heart failure (OR=1.214 [95% CI=1.050-1.403]) (all p<0.05). Other factors associated with a lower 5-year mortality included lung infection (OR=0.649 [95% CI=0.501-0.841]), NG intubation (OR=0.613 [95% CI=0.457-0.822]), and coronary artery disease (OR=0.827 [95% CI=0.705-0.972]). Because the latent groups have included significant variance of the 5-year mortality, the other variables were considered confounding factors. When we removed the latent groups from the logistic model, the coefficients of lung infection and NG intubation were changed to >1: lung infection (1.334; 1.097-1.622) and NG intubation (1.561; 1.314-1.854). The coefficient was no longer significant (0.904; 0.866-1.098) for coronary artery disease. The important characteristics exhibited by patients in cluster 3 are summarized in Figure 2.
DISCUSSION
This is the first study to show that the combination of multimorbidity and patient characteristics using LCA can predict 5-year mortality risk among a heterogeneous sample of patients with dementia. We found that a three-class solution yielded the best-fitting classification model. More specifically, we observed that the FRINGED class (i.e., cluster 3) and cardiometabolic multimorbidity class (i.e., cluster 2) were predictive of mortality within the 5-year follow-up compared to the low comorbidity burden class (i.e., cluster 1).
Based on our LCA, 13.1% of patients with dementia were classified as cluster 3, and this population had the highest 5-year mortality risk (59.6%) compared to those with a low comorbidity burden (17.6%). Stroke accounted for the largest percentage of comorbid disease in cluster 3 (82.1%), followed by NG intubation (78.7%), and COPD (70.9%). Furthermore, lung and urinary infections were also both highly prevalent in cluster 3. The clinical complexity of comorbidity among this subset of individuals with dementia poses challenges for primary and secondary care. For example, stroke is an established, strong, and modifiable risk factor for all-cause dementia [31], whereas post-stroke dementia exhibited a steep decline in global cognition compared to stroke survivors without dementia [32]. In addition, 41.3% of individuals with dementia were hospitalized due to pneumonia and urinary tract infection (UTI)—both of which are avoidable and treatable— but, nevertheless, commonly lead to markedly higher mortality [33]. The presence of coexisting comorbidities may contribute to a more negative impact on dementia management. Thus, understanding the influence of comorbidities on the pathogenesis of dementia may help prevent disease progression [34].
Patients with dementia classified into cluster 3 were similar to those with frailty, a geriatric syndrome characterized by age-related, decreased physiological reserve and increased vulnerability to stressors [35]. Studies have found that frailty is associated with an increased risk for adverse outcomes, including stroke [36], fracture [37], and infection [38]. A prospective cohort study of 1,152 community-dwelling older adults with an 18-year follow-up reported that those with frailty had a 3.78 times higher risk for mortality [39]. In addition, the prevalence of frailty among older adults living with dementia in a community-dwelling setting ranged from 24.3% to 98.9% [40]. Although frailty is not a disease per se, it profoundly influences disease expression. Dementia alone may contribute to excessive mortality, which may be further increased by comorbid frailty.
With the progression of dementia, the rate of comorbidities and severity increased. Notably, these physical comorbidities were treatable and preventable. One study reported that pneumonia, chronic heart failure, and UTI accounted for two-thirds of all potentially preventable admissions, followed by dehydration and duodenal ulcer among patients with dementia [41]. Similarly, patients with dementia are less likely to undergo treatment for hypertension [42] or age-related macular degeneration [43]. Furthermore, chronic physical conditions are frequently neglected, with 42% of unplanned admissions >70 years of age having dementia [33]. These under-diagnosed and under-treated comorbidities among patients with dementia lead to higher usage of health services, hospital admission(s), prescriptions, and mortality, particularly for patients with AD [5,44]. Understanding the inter-relationship between comorbidities and dementia is important for the development of effective, patient-tailored treatment and public health policies.
It would be difficult to compare the present findings with previous research due to differences in basic demographic characteristics and health care systems in heterogeneous populations, such as those with dementia [7,8,45]. Several factors, such as the rate of underdiagnosis of dementia, ascertainment of dates of death, medical diagnoses, and medications may introduce a high risk of bias or concerns regarding applicability [7,45,46]. Therefore, uncertainty in predicting survival probabilities remains one of the barriers to enhancing advance care planning and shared decision-making in dementia [47], particularly in an era of rising prevalence of dementia. The application of LCA in the present study yielded more information about several characteristics that may interact with one another in impacting survival. By doing this, we extended previous work that predominantly emphasized the influence of individual risk factors, such as living alone [48], increased frailty [49], and multimorbidity [50], on mortality to identify latent classes of dementia.
Several limitations of our study should be considered when interpreting our findings. First, LCA can vary over time and across cohorts; as such, additional replication and validation are required. Second, survival after diagnosis of dementia may vary according to ethnicity [51]. This study was specific to the dementia population derived from the national claims dataset in Taiwan. Thus, our findings may not be generalizable to other ethnicities. Third, the study did not distinguish among the different types of dementia [2]. Fourth, several variables, including laboratory values and lifestyle (e.g., physical activity and tobacco smoking), were not available in the dataset and may have influenced the findings.
In conclusion, the present study identified three qualitatively separate, broad multimorbidity clusters using LCA in a nationally representative Taiwanese sample of patients with dementia. We found that the different latent clusters could predict the 5-year mortality rate based on numbers of patient-and disease-specific factors. These results may inform shared decision-making practices and advance care planning in patients with dementia.