INTRODUCTION
The coronavirus disease-2019 (COVID-19) pandemic has significantly impacted people’s daily lives and entailed significant adjustments worldwide [1]. The high infection and relatively high mortality rates of COVID-19 have generated worries and concerns. Its high infectivity not only harms individual patients but also causes loss and damage to those they have come into contact with and the surrounding group, causing fears in the aftermath of cases of infection [2]. The fear of COVID-19 infection can be classified into fear for the body, fear for significant others, fear of uncertainty, and fear of taking action [3]. Most of the general public has experienced fear of transmitting COVID-19 to their families, of the absence of a definitive COVID-19 treatment, of not having complete control over COVID-19 infection, and of hearing news of confirmed cases and deaths [4].
Thus, the aspects of fear caused by COVID-19 can vary, and the greater the fear, the greater the difficulties caused by the unusual situation concerning COVID-19 [5]. Ultimately, the experience of fear of an epidemic affects many negative psychological experiences [4,6,7], and excessive fear can also negatively affect an individual’s mental health issues [8,9]. For instance, if one only stays at home, avoiding going out for fear of infection, he or she is more likely to be stressed by creating “self-isolation” rather than gaining relief from anxiety [10], and the numbers of individuals who are reluctant to go out due to fear of infection after the COVID-19 pandemic and thus suffer loneliness are increasing with increased remote classes and meetings at school or work [11]. Previous research has shown that the higher an individual’s fear of COVID-19, the higher their loneliness, ultimately harming their mental health [12].
Loneliness can be defined as an experience in which there is a discrepancy between the interpersonal relationship one wants and the interpersonal relationships one currently perceives, a deficiency one subjectively feels in social relationships, and an unpleasant and painful emotional experience [13]. Loneliness is also used in the same sense as perceived social isolation [14]. As mentioned earlier, social disconnection and isolation experienced during the COVID-19 pandemic can cause loneliness as described above [15], and there have been reports of an increase in loneliness from before the pandemic [16]. Such increased loneliness due to the pandemic can have a greater negative impact on individuals and is an issue that should be treated as more important. In particular, social isolation has been shown to be similar to those of risk factors for death, such as smoking and drinking, and to outweigh those of risk factors, such as lack of physical activity and obesity [17]. In other words, social isolation and loneliness also harm many health problems, including comorbidities, complex diseases, and mortality [14,18].
On the other hand, fear of infectious diseases can increase an individual’s emotional distress level [7]. Specifically, the greater the fear experienced due to COVID-19, the more likely an individual is to belong to the “low anxiety group” than to the “group without anxiety.” [4] Similarly, the more people worried about COVID-19 for more than three hours a day, the more likely they were to complain of anxiety disorder symptoms [19]. Fear of something that has never happened before can increase anxiety in healthy individuals as well as in those with pre-existing mental health conditions [7]. The fear of COVID-19 infection may affect anxiety itself in this way, or people may become more sensitive to interpersonal relationships or vulnerable to psychological stress as they experience anxiety due to decreased social relationships and interactions with others [20]. Specifically, it has been found that an individual’s amplified anxiety due to the prolonged COVID-19 pandemic is likely to cause a sense of isolation,15 and the higher the degree of anxiety experienced by the individual during the COVID-19 pandemic, the higher their sense of loneliness [21].
Thus, strengthening the factors that can alleviate the effects of the fear of COVID-19 infection that breeds various problems will protect individuals from psychological difficulties, such as anxiety and loneliness, during the pandemic. In particular, one can consider gratitude, one of the variables highlighted in positive psychology, which focuses on and strengthens human beings’ positive aspects. Gratitude is a state of mind of accepting benefits gained from others and objects or a moment of peaceful blessing from nature as a gift to which one responds with thankfulness and joy [22]. Such gratitude is noted for being associated with variables closely related to adaptive personality characteristics, mental health, physical health, social relationships, and spirituality [23-26]. Individuals with high levels of gratitude tend to pay attention to the positive aspects of difficult situations, and their developed awareness of feeling gratitude allows them to reinterpret the situation beneficially [27]. Specifically, people with higher levels of gratitude show higher levels of positive emotion and life satisfaction and lower levels of negative emotions such as depression, anxiety, and jealousy than those with lower levels of gratitude [24].
Gratitude has shown a positive effect on individuals who have experienced severe trauma [28], and gratitude training reduces physical symptoms and negative emotions and promotes bonding in interpersonal relationships [29]. Gratitude has also been shown to act as a protective factor against psychological stress and depression during the COVID-19 pandemic [30-32]. In addition, participating in gratitude training has been reported to lower the level of anxiety significantly [33], suggesting the possibility of controlling the relationship between the fear of COVID-19 infection and anxiety. Intervening in gratitude has the advantage that it can be done relatively easily and quickly in the clinical field [26]. If various methods and programs are put in place to promote the gratitude of individuals in intervening in psychological problems such as anxiety and loneliness during the COVID-19 pandemic, the resulting gratitude should act as a protective factor against various mental and physical diseases.
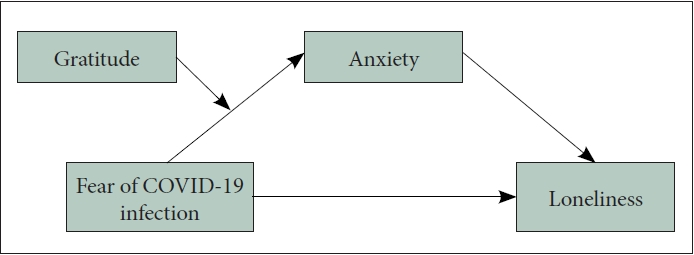
For the above reasons, this study aimed to examine the effect of fear of COVID-19 infection and anxiety on loneliness and the moderating effect of gratitude. The research hypotheses were as follows; 1) Anxiety will mediate the relationship between the fear of COVID-19 infection and loneliness. 2) Anxiety and gratitude will have a moderated mediating effect on the relationship between the fear of COVID-19 infection and loneliness. Specifically, gratitude will moderate the effect of the fear of COVID-19 infection on loneliness through anxiety. The research model is presented in Figure 1.
METHODS
Participants and data collection
The present study is a part of several mental health surveys on the psychosocial effects of COVID-19 in the general population and patients with mental disorders. For the analysis of this study, a survey was conducted among individuals aged 19 to 69 years living in three metropolitan areas. To ensure uniform age and sex distribution, quota sampling was used. The survey was conducted via a panel of online survey services (Macromill Embrain, Seoul, South Korea) on September 14-24, 2021, the second year of the pandemic, and a total of 1,500 cases were included in the analysis. Participants consented to the use of personal information before participating, and the study was approved by the Chonnam National University Hospital Institutional Review Board (CNUH-2021-297).
The 1,500 participants comprised 750 males and 750 females, with a mean age of 38.7 (standard deviation [SD]=11.9) years between 19 and 69 years. There were 816 (54.4%) single and 684 (45.6%) married participants, and 627 (41.8%) reported being religious, 873 (58.2%) not religious.
Measurement
The fear of COVID-19 infection
Seven questions on the psychological experience and stress associated with COVID-19 developed by our research team were used to measure the fear of COVID-19 infection [34]. The items are scored on a 5-point Likert scale from 1=not at all to 5=very likely. Cronbach’s α of this scale was 0.853.
Anxiety
The Generalized Anxiety Disorder-7 Scale (GAD-7), developed by Spitzer et al. [35], was used to measure anxiety. The scale consists of seven items, and respondents rate how often they have experienced such statements in the past two weeks by checking 0=not at all, 1=several days, 2=more than half the days, and 3=nearly every day. Cronbach’s α of the GAD-7 was 0.925.
Loneliness
A brief version of the UCLA Loneliness Scale, developed by Russell et al. [36] and shortened by Hughes et al. [37], was used to measure loneliness. The scale consists of three items, for which the respondents were to rate each item with 1=hardly ever, 2=some of the time, or 3=often. The Cronbach’s α of the scale was 0.855.
Gratitude
The Korean version of the Gratitude Questionnare-6 (GQ-6), which was adopted from the GQ-6, developed by McCullough et al. [24], and validated by Kwon et al. [38], was used to measure gratitude. The scale consists of six items and is scored on a 7-point Likert scale from 1=strongly disagree to 7=strongly agree. Cronbach’s α of the scale was 0.880.
Analysis procedure
The descriptive statistics were first performed to confirm the participants’ demographic information, and the correlation analysis was performed to confirm the relationship between the variables. In addition, t-tests and analysis of variance were performed to analyze differences in study variables according to sex, age, marital status, and religion among the demographic variables. Next, Model 4 of the bootstrap function in Hayes PROCESS macro [39] was applied to verify the mediating effect of anxiety in the relationship between the fear of COVID-19 infection and loneliness. Model 7 was then applied to test the moderated mediation effect of gratitude and anxiety on the relationship between fear of COVID-19 infection and loneliness. The variables were mean-centered based on the suggestions of Aiken et al. [40] to minimize multicollinearity. The IBM SPSS 23.0 (IBM Corp., Armonk, NY, USA) program was used for the statistical analysis. All statistical tests were two-tailed, and p<0.05 were considered significant.
RESULTS
Results of descriptive statistics and correlation analysis of measurement variables
The correlations, means, and SDs of the study variables are presented in Table 1. Age was significantly positively correlated with the fear of COVID-19 infection and gratitude and significantly negatively correlated with anxiety and loneliness. The fear of COVID-19 infection, the antecedent, showed significantly positive correlations with anxiety and loneliness. Anxiety, the mediator, was significantly positively correlated with loneliness and significantly negatively correlated with gratitude. Loneliness, the outcome variable, was significantly negatively correlated with gratitude.
Differences in measurement variables according to demographic variables
An independent sample t-test was performed to examine whether there were differences in the scores of each variable by sex, marital status, and religion. The analysis results of the differences in scores are presented in Table 2. The differences in the score of each variable according to sex were significant. Specifically, female respondents showed significantly higher levels of fear of COVID-19 infection, anxiety, loneliness, and gratitude than males. The scores of each variable significantly differed depending on marital status, such that the married had significantly higher fear of COVID-19 infection and gratitude and lower anxiety and loneliness than the single. The differences in the scores of the fear of COVID-19 infection and gratitude depended significantly on whether the participants had a religion or not. Those with religion showed significantly higher levels of fear of COVID-19 infection and gratitude than those without religion.
Mediating effects of anxiety in the relationship between the fear of COVID-19 infection and loneliness
The bootstrap Model 4 of PROCESS macro was applied to examine the mediating effect of anxiety in the relationship between the fear of COVID-19 infection and loneliness. Since there were differences in measurement variables according to demographic variables, sex, religion, age, and marital status were set as covariates when analyzing the models to investigate whether the models could be significantly explained even after controlling for their effects. As can be seen from Table 3, presenting the results of the mediation effect, the fear of COVID-19 infection had a significant positive effect on loneliness and anxiety. As a result of adding the fear of COVID-19 infection as a predictor and anxiety as a mediator, anxiety positively affected loneliness, the reference variable. There was a mediating effect, as the influence of the fear of COVID-19 infection on loneliness in step 1 was more significant than the influence of the fear of COVID-19 infection on loneliness when the fear of COVID-19 infection and anxiety were both applied simultaneously in step 3. Although the influence of the fear of COVID-19 infection on loneliness decreased from step 1 to step 3, the effect was still significant, and anxiety partially mediated these relationships. The bootstrap analysis showed that the indirect effect of anxiety in the relationship between the fear of COVID-19 infection and loneliness was statistically significant (B=0.040, standard error=0.006; 95% confidence interval=0.029-0.051).
Moderated mediating effects of gratitude and anxiety in the relationship between COVID-19 infection and loneliness
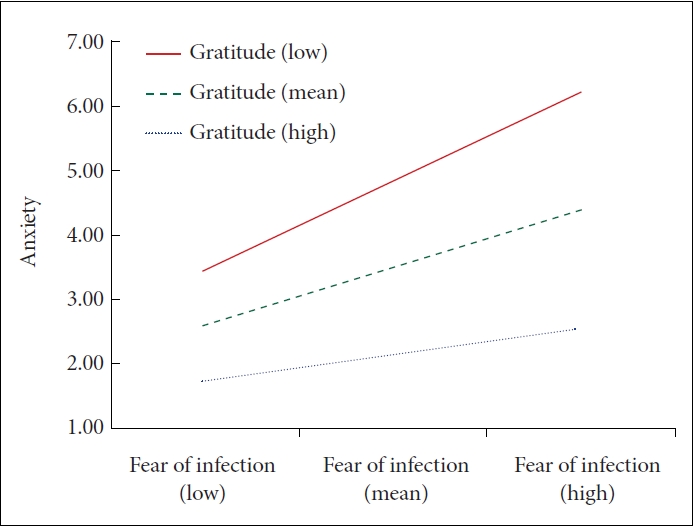
The bootstrap Model 7 of PROCESS macro was used to examine the moderated mediating effect, and sex, religion, age, and marital status were set as covariates in the model analysis. The moderated mediation effect is presented in Table 4. The interaction between the fear of COVID-19 infection and gratitude had a significant negative effect on anxiety, and anxiety had a positive effect on loneliness. In addition, the moderated mediation index of gratitude did not include 0 in the confidence interval, indicating a significant effect. These results show that the path from the fear of COVID-19 infection to loneliness through anxiety varies depending on the level of gratitude. In the analysis of the conditional indirect effect according to the level of the moderator, 0 did not fall between the lower and upper limits when the gratitude value was the mean, -1 SD, or +1 SD, and the conditional indirect effect could be interpreted as significant at all three levels. This suggests that loneliness varies according to the fear of COVID-19 infection and that the higher the gratitude, the lower the rate of increase in anxiety due to the fear of COVID-19 infection.
Figure 2 illustrates the moderating effect of gratitude, which was statistically significant. The average amount of change was examined by dividing the moderator, gratitude, into low and high groups to examine their interaction pattern, and it was found that the higher the gratitude, the lower the increase in anxiety due to the fear of COVID-19 infection.
DISCUSSION
This study examined the effect of fear of COVID-19 infection and anxiety on loneliness and the moderating effect of gratitude. It aimed to deeply understand the emotional difficulties of individuals experiencing loneliness due to the fear of COVID-19 infection and explore the possibility of utilizing gratitude, one of the most widely known protective factors, as an intervention method. Our study demonstrated that the effect of the fear of COVID-19 infection on loneliness through anxiety was moderated by gratitude.
The high levels of negative factors, such as fear of COVID-19 infection, anxiety, and loneliness, in female respondents may be due to the tendency in Korean society to accept pathological symptoms in females more readily than in males, which can be explained as a result of socialization that causes females to express or maintain symptoms more when symptoms of problems appear [41]. Furthermore, fear is subject to perceived danger, and the difference in fear of COVID-19 infection between the sexes may be the effect of females’ high detection of harm due to risk (e.g., death due to viral infection) [42]. Meanwhile, gratitude, the protective factor, was also high in females. This is inconsistent with the results of a study of Korean undergraduates who did not show sex differences in gratitude [38]. Such a difference might have been revealed in this study because the present study covered adults aged 19 to 60 years. That is, there is a possibility that the gratitude of middle-aged or older females in Korea is relatively high, thus affecting these results. In this regard, previous studies have shown that the gratitude of Korean baby boomer females is relatively high, which can be interpreted as reflecting the dynamic generational characteristics experienced by the females in the corresponding generation [43].
The fear of COVID-19 infection and gratitude were high in married participants. The fears associated with COVID-19 are not only about oneself but also altruistic fears about others, which are limited to people with whom the individual is close or acquainted [42]. Accordingly, it can be inferred that married individuals’ high level of fear of COVID-19 infection may reflect worries and concerns about their spouse or family being infected. Because gratitude can theoretically strengthen essential factors for couples, such as happiness in marriage, intimacy, and support [44], it can also be interpreted in relation to the high gratitude of the married.
For those with religion, the fear of COVID-19 infection and gratitude were high, possibly due to people’s tendency to turn to religion and spirituality to understand and respond to disasters in times of crisis [45]. Those with religion are more likely to rely upon their religious beliefs to cope with uncertainty and relieve their anxiety during a pandemic [46], and those with strong religious beliefs tend to have more gratitude [47]. Similarly, people with spiritual and religious predispositions may be more prone to experiencing gratitude [24], and spirituality and spiritual behavior have been shown to contribute to an increase in gratitude [48], indicating that spirituality and religion may be influential in promoting gratitude.
As there are differences in measurement variables by demographic variables, age, sex, religion, and marital status were set as covariates to determine whether significant results were seen even if the effects of these variables were controlled in testing the study hypotheses. The hypothesis test results showed that, first, anxiety mediated the relationship between the fear of COVID-19 infection and loneliness. The mediating effect appeared regardless of the influence of variables such as age, sex, religion, and marital status set as covariates, and a path from the fear of COVID-19 infection to loneliness through anxiety was identified. This result is consistent with prior studies showing that the fear of COVID-19 infection affects anxiety [4,19], and anxiety affects loneliness [21], indicating that anxiety, considered a type of psychological vulnerability factor, was affected by fear or infection during the COVID-19 pandemic, ultimately increasing individual loneliness.
An enduring experience of loneliness and dissatisfaction with social relationships that have lasted for at least 2 years can be distinguished by chronic loneliness [49], as chronically lonely individuals may suffer from a more extended period of interpersonal relationship deficits (e.g., cognitive, emotional, and behavioral) than those who are situationally or transiently lonely [50]. Therefore, it is necessary to pay more attention to individuals who voice chronic loneliness and to investigate the long-term effects of loneliness when the COVID-19 pandemic has lasted for over two years. The results of this study suggest that more attention should be paid to the fear of infectious diseases or infection, which can negatively affect loneliness that is directly related to individual physical and mental health and the resulting anxiety.
Second, anxiety and gratitude had a moderated mediation effect on the relationship between fear of COVID-19 infection and loneliness. Specifically, the effect of the fear of COVID-19 infection on loneliness through anxiety was moderated by gratitude. Regardless of the effect of covariates, gratitude lowered anxiety and ultimately led to lower levels of loneliness. Individuals with a heightened fear of COVID-19 infection experience more anxiety, consequently increasing their loneliness. The higher the gratitude, the more the fear of COVID-19 infection is buffered in the path to anxiety, and the lower the indirect effect on loneliness. In other words, even if the fear of COVID-19 infection is high, high gratitude is associated with lower anxiety and loneliness, consistent with previous studies showing that high gratitude is associated with low anxiety [24], and that anxiety is lowered through gratitude training [33].
Loneliness is a sign that an individual’s relationships are inadequate in some way and a key indicator of difficulty in social relationships, and lonely individuals are less satisfied with their lives [50]. Previous studies have shown that loneliness is also associated with suicidal ideation, parasuicide [51], eating disorders [52], obesity [53], sleep disorders [54], and fatigue [55]. In particular, physical distancing as a measure to alleviate pandemics has been discussed as a risk factor for loneliness that is reported to increase the risk of early death and mental and physical health conditions [16], indicating the need to strengthen gratitude as a protective factor.
As a protective factor that can buffer the development and chronicity risks of psychopathy, gratitude can be considered a broader direction of life, recognizing the positive aspects of the world [26]. In previous studies, gratitude was found to predict positive memory bias and life satisfaction [56,57], leading to higher perceptions of social support and lower stress [58]. As an intervention to increase this gratitude, one can periodically compile a gratitude list, as shown in previous studies to reduce dissatisfaction toward the body or excessive worry effectively [59,60]. Additionally, meditating, such as thinking or writing about thankful events, and delivering and reading letters of gratitude have been reported to have a positive effect [61,62]. In particular, writing a gratitude journal can increase positive emotions such as preciousness, amazement, good feelings, vitality, and positive behaviors [63]. These gratitude interventions have the advantage that they are efficient and easy to understand and implement [26]. Just as remote mental health services are actively being conducted due to the COVID-19 pandemic [64], it is believed that gratitude interventions can be easily provided through online and video media for individuals who cannot quickly receive interventions due to their fear of COVID-19 infection.
Individuals in modern society may be more vulnerable to loneliness because they lead more independent lives than in the past. Therefore, they need a more in-depth understanding of their loneliness and assistance in preventing physical and mental health problems caused by loneliness. In this regard, the current study has the significance of integrating the relationship between fear of infection, anxiety, loneliness, and gratitude during the COVID-19 pandemic. In addition, it is significant that this study explored the possibility of utilizing gratitude as a protective factor. Various gratitude intervention methods to help modern people who complain of emotional difficulties coping with stress during the prolonged COVID-19 pandemic will also greatly help prevent and resolve their mental health problems.
The fear of COVID-19 infection increased with age. This may be attributed to the higher mortality rate from COVID-19 in the elderly. One study also showed that online and written trials of gratitude interventions in which the elderly wrote about positive events and reasons for viewing them positively for two weeks had beneficial effects [65]. Using these methods to provide gratitude interventions to reduce loneliness in the elderly would be even more helpful.
A limitation of this study is that the results were obtained by analyzing cross-sectional data at a specific time. It is necessary to conduct a longitudinal study to determine the exact causal relationship between variables and the changes in variables over time. Additionally, although the positive effect of gratitude has been verified, it is not possible to know how and by what mechanism gratitude affects anxiety. Exploring the development and operating mechanism of gratitude through further research and obtaining empirical evidence will further support the adjustment of individuals suffering from pandemic anxiety and loneliness. Furthermore, as the anxiety scale used in this study measures generalized anxiety, it cannot be known what type of anxiety (e.g., health anxiety or social anxiety) specifically affected the fear of COVID-19 infection, an antecedent in this study. In addition, because of the use of self-report questionnaires, it is possible that social desirability bias affected the participants’ responses. Lastly, it is necessary to consider cultural differences in interpreting the results, as the present study only involved Koreans. There are differences in loneliness between collectivist and individualist cultures [66], and the loneliness of Koreans, who live in a collectivist culture, may differ from the loneliness experienced by people from other cultures. Therefore, the results of this study should be interpreted and applied with a consideration of the influence of culture.
In conclusion, our study demonstrated that the impact of fear of COVID-19 infection on loneliness through anxiety was moderated by gratitude. This finding points to the potential of gratitude as a protective factor in mitigating mental health issues. Gratitude interventions, which are readily accessible and effective, offer a promising avenue for the prevention and management of mental health problems, especially for individuals who may hesitate to seek immediate in-person interventions due to their fear of COVID-19 infection.