INTRODUCTION
During the coronavirus disease-2019 (COVID-19) pandemic, immunosuppressed cancer patients faced an increased risk of infection, delays in cancer treatments, and an increased fear of cancer progression [1]. The COVID-19 pandemic brought about unprecedented changes in the lives of people across the globe, as one of the primary measures taken to control the spread of the virus was to implement physical distancing [2], which was effective in reducing the transmission rate. However, this practice also resulted in delayed medical treatment for many patients, including those diagnosed with cancer [3], experiencing increased levels of anxiety and distress. The fear of contracting the virus, coupled with delays in treatments, exacerbated the stress these patients faced throughout the pandemic [4]. Moreover, the physical distancing measures had a negative impact on overall mental health [5], with a significant increase in anxiety and depression observed in society as a whole. Despite these challenges, adherence to physical distancing measures was crucial to save lives and maintain society’s overall well-being.
In contrast to healthy individuals, cancer patients are at greater risk of experiencing severe adverse events, such as intensive care admission, mechanical ventilation, and death [6]. Cancer patients may experience psychological distress related to the course of their cancer, as fear of progression or cancer recurrence is particularly distressing to cancer patients, especially as relates to delays in treatment [7]. Other forms of psychological distress which may be experienced include anxiety, depression, and post-traumatic stress disorder. Furthermore, during the COVID-19 pandemic, patients with cancer frequently experienced a fear of cancer progression, resulting from their viral anxiety related to immunosuppression [8]. In a normal, non-pandemic setting, it has been found that pretreatment fears and optimism directly predicted the recurrence of cancer after treatment [9]. Healthcare professionals should assess patients’ fear of progression and coping mechanisms, in order to reduce their fear while further developing their adaptive coping skills [10].
A cancer patient’s coping strategies can reduce psychological distress, and adaptive coping styles have been reported to be associated with lower cancer distress scores, anxiety, and depression, as well as higher quality of life scores, when compared to maladaptive coping mechanisms [11]. Among breast cancers patients, for example, depression was predicted by lower acceptance and increased catastrophizing [12]. When focusing on the general population’s response to the COVID-19 pandemic, positive thinking, actively coping with stress, and a strong support system were found to be positively associated with psychological well-being [13], while maladaptive coping strategies were reported to explain the association between increased health- and COVID-19-related anxiety [14]. Additionally, state anxiety and perceived stress during the pandemic were predicted by maladaptive emotion regulation strategies [15], while another study showed that adaptive emotional regulation mediated the relationship between the two, indicating a negative correlation between pandemic awareness and viral anxiety [16]. These results showed that coping strategies might be a significant mediator for psychological well-being among the general population during the COVID-19 pandemic.
Despite these associations, few studies have examined the effects of various coping strategies on cancer patients’ viral anxiety or depression during the COVID-19 pandemic. We found, in particular, no studies which explored the mediating effects of coping strategies on the association of cancer patients’ fear of progression and their viral anxiety or depression. In the present study, therefore, we explored whether symptoms of viral anxiety and depression are associated with a fear of cancer progression. We also assessed whether or not coping strategies utilized in response to fear of progression affected patients’ viral anxiety or depression. We hypothesized that: 1) fear of cancer progression may be associated with viral anxiety; 2) fear of anxiety may be associated with depression; 3) adaptive coping strategies may, at least partially, mediate the relationship of fear of progression with viral anxiety or depression; and 4) maladaptive coping strategies may, at least partially, mediate the relationship of fear of progression with viral anxiety or depression.
METHODS
Patients and study design
The present study was a cross-sectional survey involving cancer patients who visited Ulsan University Hospital in Ulsan, Korea between December 7, 2020 and February 9, 2021. Participants who provided written informed consent were enrolled in the study, and voluntarily responded to a survey form, which included questions regarding each participant’s age, sex, marital status, educational level, religion, occupation, current alcohol and/or tobacco use, past psychiatric illness, and cancer type, stage, treatment, and remission status. As an incentive for their participation, participants were offered an e-gift coupon valued at $5. The protocol for the present study was approved by the Institutional Review Board of Ulsan University Hospital (IRB 2020-1055).
Rating scales
Stress and Anxiety to Viral Epidemic-6
The Stress and Anxiety to Viral Epidemic-6 (SAVE-6) rating scale is utilized for assessing one’s anxiety response to the COVID-19 pandemic [17]. It is a subcategory of the SAVE-9 scale, which was originally developed for evaluating healthcare workers’ stress and anxiety in response to viral epidemics [18]. The SAVE-6 scale was evaluated, and while it was already administered to cancer patients, it was confirmed to be applicable to the general population [19]. Respondents answer the 6 items of the SAVE-6 using a 5-point scale, which ranges from 0 (never) to 4 (always), and a higher score correlates to an increased degree of anxiety response to viral epidemics. The cutoff score has been defined as ≥15, corresponding to at least a mild degree of generalized anxiety (Generalized Anxiety Disorder-7 scale, score ≥5) among the general population, and is compatible to a result of at least moderate functional impairment, based on the Work and Social Adjustment Scale score (≥11) among cancer patients [20]. In this study, the original version of the SAVE-6 which was developed in Korean language was applied [17], and Cronbach’s α among this sample was 0.819.
Patient Health Questionnaire-9
The Patient Health Questionnaire-9 (PHQ-9) rating scale is utilized for measuring the severity of one’s depressive symptoms [21]. It is a self-rating scale consisting of 9 items scored using a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day), and a higher score corresponds to a greater degree of depression (0-4, minimal depression; 5-9, mild depression; 10-14, moderate depression; 15-19, moderately severe depression; and ≥20, severe depression). For the present study, we used the Korean version of the PHQ-9 [22], and defined clinical depression as a score of ≥10. Cronbach’s α among this sample was 0.851.
Cognitive Emotion Regulation Questionnaire-short version
The Cognitive Emotion Regulation Questionnaire (CERQ) rating scale is utilized for measuring cognitive coping strategies, and consists of five adaptive emotional regulation strategies (acceptance, positive refocusing, positive reappraisal, putting into perspective, and refocus on planning) and four maladaptive emotional regulation strategies (self-blame, blaming others, rumination, and catastrophizing) [23]. For the present study, we used a Korean validated 18-item short version of the CERQ (CERQ-18) [24]. Cronbach’s α among this sample was 0.885.
Fear of Progression Questionnaire-short version
The Fear of Progression Questionnaire (FoP-Q) is a 43-item rating scale utilized for evaluating concerns related to disease progression. For the present study, we used the Korean validated 12-item short version (FoP-Q-SF) [25], on which each of the 12 items are rated from 1-5. Cronbach’s α among this sample was 0.911.
Statistical analyses
The participants’ clinical characteristics were summarized as mean±standard deviation, and the level of significance for all analyses was defined as a two-tailed p-value <0.05. In the step 1, we performed a stepwise linear regression analysis to explore whether fear of progression, viral anxiety, or depression in cancer patients was expected by adaptive or maladaptive coping style. In the step 2, we performed a linear regression analysis with the enter method to evaluate predictive variables for fear of progression in cancer patients, including all subscales of coping strategies which was significant in step 1, viral anxiety, and depression. In the step 3, we performed the bootstrap method with 2,000 resamples to evaluate the mediation effect of coping strategies, which was significant in step 2, on the association of fear of progression with viral anxiety or depression. Statistical analyses were performed using the AMOS ver. 28 package (IMB Corp., Armonk, NY, USA) and IBM SPSS ver. 21.0 for Windows (IBM Corp.) and jamovi 2.2.5 (https://www.jamovi.org).
RESULTS
Among the 558 cancer patients who participated in the present study, 281 (50.4%) were male, 164 (29.4%) were working, 279 (50.0%) were diagnosed as having solid cancers, 402 (72.0%) were undergoing treatment, 106 (19.0%) were in complete remission (Table 1), and 25 (4.5%) reported that their treatment schedule was delayed during the COVID-19 pandemic (Supplementary Table 1 in the online-only Data Supplement). Among the “delayed” and “as scheduled” treatment groups, the number of patients who were actively drinking alcohol or had psychiatric illnesses was significantly higher in the “delayed” group, while the number of patients actively undergoing cancer treatment was significantly higher in the “as scheduled” group. Viral anxiety, measured with the SAVE-6, was marginally more severe (p=0.06), while depression, assessed with the PHQ-9, fear of disease progression, measured with the FoP-Q-SF, and maladaptive coping strategies, rated with the CERQ-18, were significantly higher in the “delayed” group.
During the analyses, we first performed a stepwise linear regression analysis using age, symptoms rating scales, and coping strategies (adaptive and maladaptive coping), as seen in Table 2. Fear of progression in cancer patients was predicted by depression (PHQ-9, β=0.25; p<0.001), viral anxiety (SAVE-6, β=0.42; p<0.001), and maladaptive coping strategies (CERQ-18, β=0.17; p<0.001). Viral anxiety in cancer patients was predicted by fear of progression (β=0.56; p<0.001) and adaptive coping strategies (β=-0.10; p=0.008). Depression in cancer patients was predicted by fear of progression (β=0.35; p<0.001), adaptive (β=-0.14; p<0.001), and maladaptive (β=0.32; p<0.001) coping strategies.
We next performed a stepwise linear regression analysis using age, symptoms rating scales, and four maladaptive coping strategies subscales to explore variables which might predict cancer patients’ fear of progression (Table 3). This analysis showed that fear of progression in cancer patients was expected by age (β=-0.08; p=0.011), viral anxiety (β=0.40; p<0.001), depression (β=0.26; p<0.001), and catastrophizing coping strategies (β=0.15; p=0.004), for an overall adjusted R2 of 0.46 (F=66.8; p<0.001).
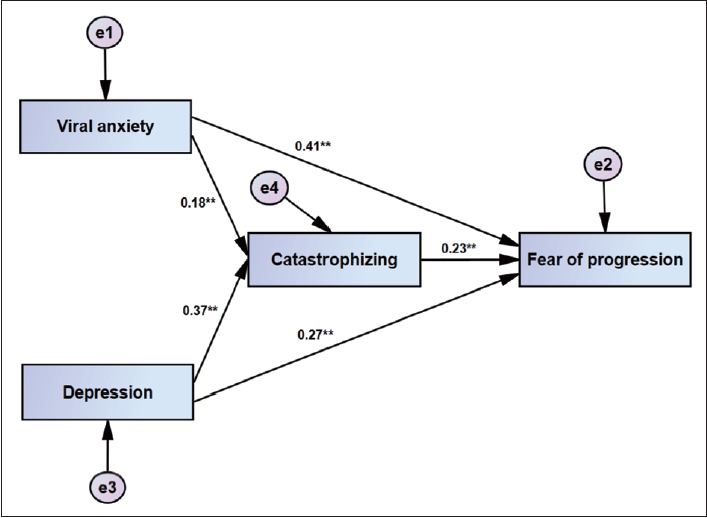
Lastly, we performed a mediation analysis to evaluate whether or not catastrophizing, as a maladaptive coping strategy, mediates the relationshop of depression or viral anxiety with fear of progression among cancer patients (Table 4 and Figure 1). Through this analysis, we observed that viral anxiety and depression directly associated with fear of progression in cancer patients, and that catastrophizing mediated this relationship.
DISCUSSION
In the present study, we found that fear of progression in cancer patients during the COVID-19 pandemic was predicted by depression, viral anxiety, and maladaptive coping strategies (catastrophizing). Viral anxiety and depression were directly associated with fear of progression in cancer patients, and catastrophizing, as a maladaptive coping strategy, mediated this relationship. During the first wave of COVID-19 in 2020, many cancer patients experienced delays in diagnosis and/or treatment [3], due to the need to divert resources to care for COVID-19 patients, which caused many cancer clinics and hospitals to reduce their capacity to treat patients, or even close temporarily. For cancer patients, this caused delays in not only obtaining a diagnosis, but also in the availability of chemotherapy, radiation therapy, and surgery. Due to these delays, patients may have experienced psychological distress, such as anxiety, depression, or fear of disease progression.
In the present study, we found that less adaptive coping strategies were associated with increased viral anxiety or depression, while in the relevant literature, among breast cancer patients in particular, we previously reported that less acceptance (an adaptive strategy) predicted an increased level of depression [12]. Additionally, the presence of maladaptive coping techniques was indicative of increased fear of progression and depression. Similarly, in a previous study of patients with breast cancer, it was reported that fear of progression was associated with maladaptive coping strategies, such as avoidance and self-punishment [10]. Fear of progression in cancer patients was predicted by viral anxiety, depression, and/or catastrophizing, as a maladaptive coping strategy. We did not include, in the present study, whether or not a patient’s treatment schedule had been delayed as a confounding variable in the mediation model, since the proportion of delayed patients is low (4.5%).
The survey was conducted between December 7, 2020 and February 9, 2021, approximately one year after the first outbreak of COVID-19. While 80,000 people had been infected and 1,500 had died as a result of the COVID-19 pandemic at the time [26], people were able to adjust to the situation. Although the healthcare system is still responsible for caring for infected patients, most hospitals are taking care of cancer patients on a regular basis. It may be a reason for the low proportion of delayed patients. However, we did observe that patients whose schedules were delayed showed an increased level of depression, viral anxiety, or fear of progression. In the first wave of the COVID-19 pandemic, cancer patients who had their treatment schedules delayed suffered from worries about viral infections and fears that their disease would progress as a result of the delayed treatment, subsequently resulting in depression symptoms.
Additionally, in the present study, we observed that the use of catastrophizing as a coping strategy mediated the relationship of depression and viral anxiety with fear of progression in cancer patients. Similar to the results of a previous study [8], the results of the present study indicated a significant relationship between viral anxiety, depression, and fear of progression. During the COVID-19 pandemic, cancer patients’ fear of progression was found to be related to viral anxiety. Many cancer patients were more fearful of COVID-19 than they are of the actual disease [27]. We also previously reported that functional impairment observed in cancer patients was predicted by an increased fear of COVID-19 over the actual cancer [3]. As a high-risk group, cancer patients are more susceptible to COVID-19, and as a result of their impaired immune function, patients believe that infection might be more likely. In some cases, these beliefs can be linked with misguided beliefs about sleep, indicating that cancer patients with insomnia may also experience impaired immune function, which increases their risk of infection [27]. A significant correlation was also found between depression and fear of progression among cancer patients during the COVID-19 pandemic, in which the fear of cancer progression can potentially lead to an increase in symptoms of depression, such as sadness, hopelessness, and loss of interest in life. On the other hand, patients who suffer from depression may find it more difficult to cope with the fear of their disease progressing. Considering the fact that depression can exacerbate feelings of hopelessness and anxiety about the future, patients experiencing depression may become more concerned about their cancer prognosis as well as the impact of the pandemic on their health.
In the present study, the use of catastrophizing, as a coping strategy, was found to mediate the association of viral anxiety or depression with fear of progression in cancer patients. As a cognitive distortion, catastrophizing, the process of ruminating, magnifying, and feeling helpless, is associated with painful events [28], and the tendency to magnify and feel helpless increases with catastrophizing [29]. During the COVID-19 pandemic, cancer survivors reported greater COVID-related catastrophizing than healthy controls [30]. We hypothesized that the use of catastrophizing as a maladaptive coping strategy might enhance cancer patients’ fear of progression, by mediating their viral anxiety. In a previous study, we observed that cancer-related misguided beliefs about sleep mediated the association of viral anxiety and depression with fear of progression [8]. Misguided beliefs about sleep also include the meaning of catastrophizing [31], indicating that ruminating or increased worrisome feelings during the COVID-19 pandemic might enhance fear of progression among cancer patients.
There are several limitations in this study. First of all, this study was done among cancer patients in a single tertiary general hospital located in Ulsan. The interpretation of these results should be done with caution. Second, we could not collect the responses of being infected or quarantined in this study. The proportion of infected patients might influence the results. Third, this study is based on a cross-sectional survey, which does not provide information regarding the temporal precedence of the mediation model. Whenever the results are interpreted, caution should be exercised.
In conclusion, as a result of the delay in the diagnosis and/or treatment of cancer due to the COVID-19 pandemic, cancer patients suffer increased psychological distress, including a fear of the progression of their disease. We found, in the present study, that during the COVID-19 pandemic, fear of progression in cancer patients can be associated with viral anxiety, depression, and maladaptive coping techniques, such as catastrophizing. Based on the results of the present study, healthcare providers should consider the psychological impact of the COVID-19 pandemic on cancer patients, and provide the appropriate support and interventions. In order to do this, we may need to address maladaptive coping strategies, provide mental health resources, and ensure that cancer diagnoses and treatments are made available in a timely manner. Furthermore, public health measures should prioritize the safety and treatment of cancer patients during pandemics and other crises, in order to minimize disruptions to their health care.