INTRODUCTION
Patients encountered in clinical practice commonly complain of insomnia [1-3]. Cognitive-Behavioral Therapy for insomnia (CBT-I) is recommended as the first line of treatment for insomnia, but it requires enough time and education for the therapist to be effective [4,5]. Clinically, this is difficult for physicians, especially those who are well unacquainted with CBT, to treat many patients in a limited amount of time. Therefore, simple instructions, which can effectively reduce patients’ insomnia symptoms, are needed.
We previously reported the DBST index, the discrepancy between desired time in bed (dTIB) and desired total sleep time (dTST), and its relationship with insomnia severity among the general population and cancer patients [6-8]. For example, if a patient desperately wants to sleep at least 5 h (5 h of dTST), but they want to sleep from 9 PM to 7 AM (10 h of dTIB), we can estimate the DBST index as 5 (10 h of dTIB-5 h of dTST). Originally, the concept of the DBST index was developed based on the findings that insomnia patients desire desperately to sleep for at least a short period, but unconsciously desire a greater amount of time to sleep [4,9]. We hypothesized that patients who have more severe insomnia may have a higher DBST index than others. And, we observed that the DBST index was significantly associated with the insomnia severity measured with the Insomnia Severity Index (ISI) among the general population [6,8]. Our results showed the possibility of using the DBST index as a simple index, which can predict the insomnia severity, despite being unable to report the study done in the patients with insomnia.
However, no study has explored the relationship between change in the DBST index and change in insomnia severity. To lower one’s DBST index, one must reduce the time one wants to spend in bed (dTIB). A reduction in dTIB may decrease the discrepancy between dTIB and dTST and increase sleep efficiency, which is a measure of TST over TIB [10]. An individual may experience fewer sleep disturbances because of improved sleep efficiency. Conversely, an increase in DBST means that dTIB was increased or dTST was decreased. When dTIB increases, sleep efficiency may be reduced, which can result in sleep disturbances. Therefore, it is theoretically possible that change in the DBST index would be related with change in the insomnia severity.
However, the cognitive therapy domain is one of the most important components of the CBT-I [4,11-13]. The relationship between the DBST index and cognitive domains such as dysfunctional beliefs about or preoccupation with sleep was explored. We observed that the DBST index was significantly correlated with preoccupation with sleep measured with the Glasgow Sleep Effort Scale (GSES) [6] or dysfunctional beliefs about sleep measured with the Dysfunctional Beliefs and Attitude about Sleep-16 items (DBAS-16) scale [8]. These studies showed that the influence of the DBST index on the insomnia severity was mediated by preoccupation with or dysfunctional beliefs about sleep. However, we are still unsure whether a change in DBST index can be achieved through changes in dysfunctional beliefs about or preoccupation with sleep, though we observed that the influence of the DBST index on insomnia severity was mediated by preoccupation with [6] and dysfunctional beliefs about sleep [8]. Can a change in the DBST index through an increase or decrease in the dTIB cause a change in preoccupation with or dysfunctional beliefs about sleep?
In this study, we aimed to explore whether the change in DBST index is significantly correlated with change in insomnia severity. Additionally, we explored whether the change in the DBST index is significantly associated with change in degree of preoccupation with or dysfunctional beliefs about sleep. We posited that 1) change in the DBST index from first survey (T1) to second survey (T2) will be correlated with the change in insomnia severity from T1 to T2 survey, 2) change in the DBST index will be correlated with a change in preoccupation with sleep, 3) change in the DBST index will be correlated with a change in dysfunctional beliefs about sleep, 4) the influence of change in the DBST index on change in insomnia severity will be mediated by a change in preoccupation with sleep, and 5) the influence of change in the DBST index on a change in insomnia severity will be mediated by change in dysfunctional beliefs about sleep.
METHODS
Participants and procedure
A survey and follow-up survey were conducted, in which participants aged 18-60 years old responded to the T1, followed by a T2 approximately 6 weeks later. We asked participants to complete both the T1 and T2 surveys, and those who agreed were enrolled in the T1 survey. The T1 survey was completed by all 400 participants between the 26th and 30th of September, 2022, and the T2 survey by 234 (58.5%) of those participants between the 5th and 16th of November, 2022. The anonymous online survey was conducted using an online platform provided by the company EMBRAIN (Seoul, Korea). Participants were drawn from the 1,640,000 registered panelists of the company.
The required sample size for the T1 survey was estimated based on allocation of 50 samples for 8 cells (biological sex× four age groups [20’, 30’, 40’, and 50’]) [14]. In the T1 survey, enrollment emails were sent to 7,195 participants, 1,021 accessed the survey, and 460 completed it. After excluding incomplete and too fast responses, the first 400 responses were delivered to researchers without identifying information. We analyzed the data of 399 responses after excluding 1 due to inappropriate responses to the questions of sleep indices. In the T2 survey, enrollment emails were sent to the 400 participants of the T1 survey, 316 accessed the survey, and 242 completed it. All 233 responses, after excluding incomplete responses, were delivered to researchers.
In the forms of the T1 and T2 surveys, questions on age, sex, marital status, past psychiatric history, and current psychiatric distress were included. Rating scales and questions on participants’ sleep patterns were also included. When participants completed the T1 survey, the following question was posed to participants: “For a good night’s sleep, you should adjust your desired bedtime and desired wake-up time according to your desired total sleep time. Thus, if you desire to sleep 7 hours, you should go to bed at 11 PM and get up at 6 AM, or go to bed at 12 AM and get up at 7 AM. The result will be 7 hours of sleep.” The T2 survey was completed 5-6 weeks after the T1 survey. The study protocol was approved by the Institutional Review Board of Asan Medical Center (2022-1283). The need for written informed consent was waived. Nevertheless, surveys were conducted among participants who agreed to participate and selected “yes” to the enrollment statement stating that there would be both T1 and T2 surveys.
Measures
Sleep indices and the DBST index
Calculating the time variables
Questions such as “What is your usual bedtime?”, “What is your usual time to fall asleep?”, and “What is your usual time to finally get out of bed in the morning?” were included in the survey to calculate participants’ time variables of sleep indices such as bedtime, sleep onset time, or wake-up time. These were estimated by averaging the usual times participants responded. If a participant answered that their usual bedtime was between 22:30 and 23:00, the estimated usual bedtime was 22:45. Time variables were transformed into numeric variables for statistical analysis. Any answers of 15 min (one quarter of an hour) were converted to 0.25 (one quarter) and 30 min (half an hour) were converted to 0.50. In this manner, 22:45 was transformed into 10.75 [15,16].
Calculating duration variables
Using the estimated time variables, duration variables were calculated. Sleep onset latency (SOL) was calculated by subtracting bedtime from sleep onset time. TIB was calculated by taking the difference between the wake-up time and the bedtime (TIB=wake-up time + 12 - bedtime). We also estimated patients’ duration from wake-up time to bed time (WTB, 24-TIB) [17]. The time in bed during 24 h (TIB/d) [9] was also estimated based on responses to questions of “How long do you stay lying down on your bed during a day?”.
Calculating the DBST index
The DBST index was calculated as the difference in the patient’s dTST estimated based on the response to the question “How many hours do you wish to sleep a day?” and a dTST as determined by responding to the question “From what time to what time do you wish to sleep?”. The DBST index was calculated as [desired hours of time in bed]-[desired hours of total sleep time] [8].
ISI
The ISI is a self-rating scale designed to measure the severity of insomnia in an individual [18]. It includes seven items, and an increase in the total score indicates a more severe level of insomnia. Cronbach’s α among T1 and T2 samples was 0.844 and 0.810, respectively.
GSES
The GSES is a self-rating scale designed to measure preoccupation with sleep in an individual [19]. It contains seven items, and these can be rated on a 3-point Likert scale (0: not at all, 1: some extent, 2: very much). A higher total score indicates that someone made greater effort to fall asleep. In this study, Cronbach’s α among T1 and T2 samples were 0.827 and 0.812, respectively.
Dysfunctional Beliefs about Sleep-2 items scale
The Dysfunctional Beliefs about Sleep-2 items scale (DBS-2) is a self-report scale designed to measure dysfunctional beliefs about sleep in an individual [20]. It contains two items, and these can be rated on a 0-10 scale. A higher total score indicates a greater level of dysfunctional beliefs about sleep. In this study, the original Korean version of the scale was applied, and split-half coefficients among T1 and T2 samples were 0.844 and 0.845, respectively.
Statistical analysis
We aimed to explore whether the change in the DBST index is correlated with the change in insomnia severity among the general population. First, we examined the Pearson’s correlation coefficient among the DBST index, insomnia severity, and other rating scales in each survey (T1 [n=399] and T2 [n=233]). Second, we conducted a paired t-test for rating scales and sleep indices among the 233 participants who completed T1 and T2 surveys. Third, using the delta (Δ) value of each variable (T1-T2), we examined Pearson’s correlation coefficients among the DBST index, insomnia severity, and other variables. Fourth, linear regression analysis with enter methods was run to explore expecting variables for change in insomnia severity or the DBST index using change in each variable. Last, to explore which variables mediate the influence of the DBST index on insomnia severity, the bootstrap method with 2,000 resamples was applied to conduct the mediation analysis. Demographic characteristics and rating scale scores were summarized using the mean±standard deviation. A significance level of p<0.05 was established for all analyses. The software used to conduct the statistical analysis were IBM SPSS version 21.0 (IBM Corp., Armonk, NY, USA), AMOS version 27 (IBM Corp.), and JASP version 0.17.1.0 (JASP teams, Amsterdam, The Netherlands).
RESULTS
Demographic characteristics and rating scale scores of the T1 (n=399) and T2 (n=233) survey are presented in Table 1. In the T1 survey, the ISI was significantly correlated with GSES (r=0.55, p<0.001), DBS-2 (r=0.22, p<0.001), and the DBST index (r=0.14, p<0.01). The DBST index was significantly correlated with the dTST (r=-0.40, p<0.001), desired bedtime (r=-0.48, p<0.001), desired wake-up time (r=0.41, p<0.001), and dTIB (r=0.70, p<0.001) (Table 2). At T2 survey conducted 5-6 weeks after the T1 survey, the ISI was significantly correlated with GSES (r=0.67, p<0.001), DBS-2 (r=0.20, p<0.001), desired bedtime (r=-0.16, p<0.05), desired TIB (r=0.17, p<0.05), and the DBST index (r=0.22, p<0.01). The DBST index was significantly correlated with the GSES (r=0.16, p<0.05), dTST (r=-0.51, p<0.001), desired bedtime (r=-0.45, p<0.001), desired wake-up time (r=0.26, p<0.001), and dTIB (r=0.61, p<0.001).
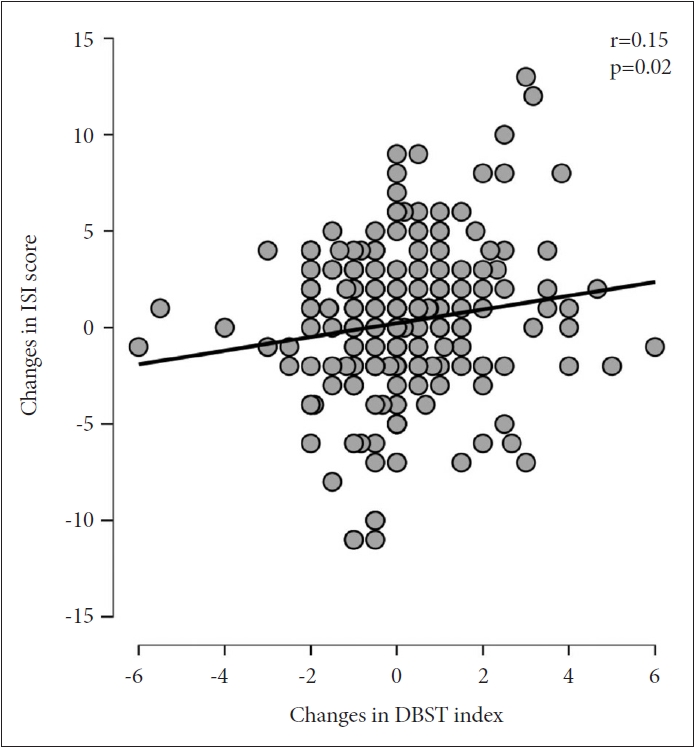
In Table 3, rating scale scores and sleep indices at baseline (T1) and follow-up (T2) surveys among participants who responded to both of two surveys are presented. Paired t-test results showed there are no significant changes in rating scales scores and sleep indices between T1 and T2 surveys (n=233). There was no significant difference in sex (p=0.860), age (p=0.894), scores of the ISI (p=0.401), DBS-2 (p=0.504), GESE (p=0.654), or DBST index (p=0.775) at baseline between participats who completed T2 survey or not. Table 4 shows the correlation coefficients among changes in each rating scale and change in the DBST index. The decrease in the ISI (T1-T2) was significantly correlated with the decrease in the GSES (r=0.24, p<0.001), DBS-2 (r=0.22, p<0.001), and DBST index (r=0.15, p=0.020) (Figure 1). The decrease in the DBST index were significantly correlated with increase in dTST (r=-0.50, p<0.001), delayed dBT (r=-0.51, p<0.001), advanced desired wake-up time (r=0.32, p<0.001), and decrease in dTIB (r=0.58, p<0.001).
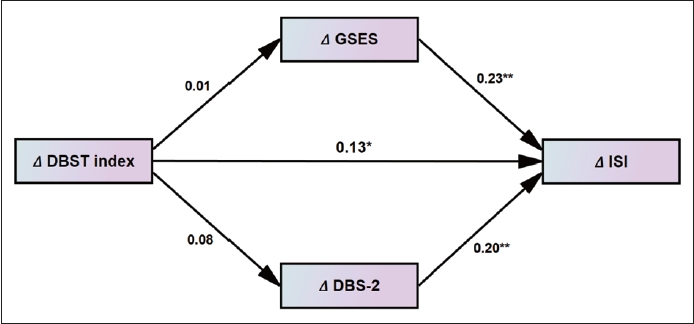
Table 5 shows linear regression analysis results. The decrease in insomnia severity was expected with decrease in the GSES (β=0.23, p<0.001), DBS-2 (β=0.20, p=0.002), and DBST index (β=0.13, p=0.037). The decrease in DBST index was only predicted by decrease in insomnia severity (β=0.14, p=0.036). Mediation analysis (Table 6 and Figure 2) showed that decrease in DBST index directly influenced decrease in insomnia severity and change in GSES or DBS-2 did not mediate the relationship (Figure 2).
DISCUSSION
In this study, we observed that insomnia severity was significantly correlated with the DBST index of T1 and T2 surveys. Among 233 participants who completed both the T1 and T2 surveys, change in DBST index was significantly correlated with change in insomnia severity. The change in insomnia severity was expected by change in preoccupation with sleep (GSES), dysfunctional beliefs about sleep (DBS-2), and the DBST index in the linear regression analysis. The change in insomnia severity was influenced by the DBST index but change in preoccupation with and dysfunctional beliefs about sleep did not mediate the relationship.
In this study, insomnia severity was correlated with the DBST index in each survey in accordance with the previous studies [6,8]. The concept of DBST is based on the idea that an individual with a sleep problem often goes to bed too early in the evening [17]. Since they cannot easily fall asleep, they believe that an early bedtime will result in a good night’s sleep. Still, early sleep can be achieved in conjunction with an early wake-up [21,22]. Previously, we observed that the WTB was significantly longer among patients whose sleep latency was ≤30 min than those with a sleep latency of >30 min [17]. Early bedtime might be associated with a long SOL. Discrepancy between dysfunctionally unconscious long TIB and desperately short total sleep time may lead to insomnia severity.
This is the first report exploring whether change in DBST index is significantly correlated with change in insomnia severity. A change (reduction) in the DBST index means that an individual reduces the amount of TIB that they want to obtain. It is well known that reduced TIB is related with increased sleep efficiency [10,23]. Therefore, our results show the possibility that reducing the discrepancy between dTIB and dTST may reduce insomnia severity. Additionally, there was significant correlation between the insomnia severity and the DBST index in the T2 survey, done 5-6 weeks after the T1 survey and providing the instruction of reducing the discrepancy. We can consider that insomnia severity may be changed when the DBST index is changed. Despite this, our results should be interpreted with caution. First, we provide information on an instruction that reducing the discrepancy may lead to good sleep, when they complete the T1 survey. However, we could not confirm that all participants had read the instructions correctly. Furthermore, we could not check whether participants tried following this instruction during the 5-6 weeks between T1 and T2 surveys. Consequently, we cannot conclude that participants intentionally reduced their discrepancy and felt that their insomnia severity had improved. Second, there was no significant difference in rating scales scores and sleep indices between the T1 and T2 surveys in paired t-tests. This means that some participants’ insomnia severity was improved, but some found that their insomnia was aggravated. Additionally, sleep indices, including the DBST index and its components, may be delayed, advanced, shortened, or lengthened individually. However, we could not clearly cut and categorize participants, and could not see the real effect of reduction of the DBST index on reducing insomnia severity.
In this study, the change in DBST index was not related with change in preoccupation with or dysfunctional beliefs about sleep. Additionally, changes in preoccupation with or dysfunctional beliefs about sleep did not mediate the influence of the change in the DBST index on the change in insomnia severity. The reason for this can be explained as follows: first, reducing the DBST index is a behavioral component, rather than a cognitive technique, similar to the sleep restriction therapy of the CBT-I [4]. The sleep restriction technique is a strategy aimed at improving sleep efficiency by reducing the time spent in bed while awake. Reducing the DBST index is also a technique that involves establishing a strict sleep schedule that limits the time in bed to only the amount of total sleep time needed for adequate sleep an individual desires. Second, it is possible that a change in preoccupation with or dysfunctional beliefs about sleep is not particularly effective in improving insomnia severity. Reportedly, improved dysfunctional beliefs about sleep after the CBT-I did not play a crucial role in reducing insomnia severity [24,25], despite several reports of positive results [26,27]. In this study, however, we observed that change in insomnia severity was significantly associated with change in sleep-related cognitions. The explanations provided above lead us to conclude that decreasing the DBST index is the only behavior technique that can reduce insomnia severity independently of the cognitive component of CBT-I.
However, the meaning of these results should be interpreted with caution. In the T1 survey, the DBST index was not significantly correlated with the GSES and DBS-2 scales scores. In the T2 survey, the DBST index was weakly correlated with the GSES scales (r=0.16, p<0.05). Additionally, change in DBST index was not correlated with changes in GSES and DBS-2 scores. In previous studies, the DBST index was significantly correlated with the GSES 6 among the general population. We reported that preoccupation with [6] and dysfunctional beliefs about [8] sleep mediate the influence of the DBST index on insomnia severity, which shows the possibility that changes in those scales may be correlated with each other. However, we could not observe the mediating effects of changes in the GSES and DBS-2 on the effect of changes in the DBST index on changes in ISI. The difference in characteristics of these samples might influence these results.
There were several limitations in this study. First, this study was done via anonymous online survey, not face-to-face clinical interviews. We could not confirm whether participants understood the exact meaning of questions on the DBST index and its components. This possible misunderstanding may lead to bias in this study. Second, we conceptually tried an intervention between T1 and T2 surveys using a simple instruction of reducing the DBST index, but maybe the instruction was not well delivered to participants. Third, this study was done among the general population rather than in patients with clinical insomnia. There is a need for further research involving patients having insomnia with better explanations, clearly asking them their sleep indices and the DBST index and good guidance to reduce the discrepancy and follow up on the changes.
Despite these limitations, this study indicates there is a possibility that insomnia severity can be changed in accordance with the changes in the DBST index even among the general population. We conclude that change in DBST index can lead to changes in insomnia severity without the mediation effect of changes in cognitive domains such as preoccupation with or dysfunctional beliefs about sleep. After a more detailed clinical study, we hope that insomnia severity of patients with insomnia can be reduced by a simple instruction that reduces the DBST index.