Effectiveness of Gatekeeper Training for Families of People With Mental Disorders in Korea: A Randomized Controlled Trial
Article information

Abstract
Objective
Given the high suicide risk among people with schizophrenia and other mental disorders and the significance of intervention in the daily life setting, tailored gatekeeper training is necessary for families of people with mental disorders. This study evaluated the effectiveness of a suicide prevention education program for families of people with mental disorders (SPEM-F), developed by the Korea Foundation for Suicide Prevention.
Methods
Fifty-nine family members of people with mental disorders were recruited from eight community psychiatric rehabilitation centers in Korea and enrolled in a cluster randomized controlled trial. Four facilities were randomized to the experimental group (n=30) and four to the control group (n=29). The study parameters were measured at baseline, post-intervention, and 1-month follow-up; the effects of SPEM-F (90 minutes, conducted offline) were analyzed using repeated-measures analysis of variance. The dependent variables were suicide-related knowledge, attitude, self-efficacy, preventive behavioral intention, and family problem-solving communication.
Results
The experimental group showed significant increases in suicide-related knowledge (p<0.001), self-efficacy (p<0.05), and preventive behavioral intention (p<0.01) compared with the control group until the 1-month follow-up, including an upward trend in improved family problem-solving communication (p=0.069).
Conclusion
The results confirm that SPEM-F is an effective evidence-based gatekeeper training program for families of people with mental disorders, as it focuses on knowledge, self-efficacy, preventive behavioral intention, and communication improvement. As families of people with mental disorders including schizophrenia, are both highly motivated and close to people at high risk for suicide, SPEM-F can effectively promote suicide prevention and gatekeeper activities.
INTRODUCTION
People with mental disorders (PMDs) are at an elevated risk for suicide compared with the general population. In Korea, the suicide rate per 100,000 population among PMDs (122.4 persons) is 4.7 times higher than that in the total suicide rate per 100,000 population (26.0 persons) [1]. Alarmingly, the rate of suicide per 100,000 population within one year of schizophrenia diagnosis (600 persons, 0.60%) is 23 times higher than the total suicide rate per 100,000 population in Korea, being higher than the overseas psychosis-related suicide rate (0.48%) [2,3]. A survey of all registered members of mental health institutes in Korea has revealed that more than half of all members (48,830 of 93,522) have severe mental disorders, namely, schizophrenia, major depressive disorder, and bipolar disorder [4]. Moreover, a survey of registered members with severe mental disorders in Seoul, Gyeonggi-do, Daegu, and Busan, Korea, found that 30%–40% of the members have a history of suicide attempts [5-8]. Protective factors for suicide among PMDs are currently under-researched in comparison to risk factors; individual therapy and family education appear to be the only intervention options available [9].
Among the available interventions, family education has been shown to promote treatment adherence and suicide prevention in PMDs. PMDs require meticulous management in their daily living to ensure treatment adherence; family cooperation is essential for this purpose, as health care professionals alone cannot continue keeping patients on their treatment regimen [10]. Given that the risk of suicide in PMDs including schizophrenia, tends to increase after hospital discharge, the role of family members is particularly critical in closely observing the patient’s condition, evaluating suicide risk, and facilitating patient referrals to health care institutions, if necessary, from the moment of discharge. However, studies have tended to emphasize the role of family members in the care of PMDs without proposing concrete methods for communication and support to prevent suicide.
Despite their desire to empathize with their loved ones, family members of PMDs often struggle with communication difficulties. PMDs often fear negative evaluations from others and may not clearly articulate their symptoms or suicidal ideation, instead preferring to subtly show suicide warning signs to family members or others around them [11]. Therefore, tailored gatekeeper training for families may enhance family members’ ability to recognize suicide warning signs in the daily lives of PMDs and provide prompt assistance.
Gatekeeper training is a universal suicide prevention education program. It provides participants (gatekeepers) with knowledge, skills, and practical methods to recognize and intervene with people at high risk of suicide and refer them to mental health services as necessary. People at high risk of suicide tend to fear social stigma and hesitate to seek help, instead preferring to subtly express their emotional distress to their friends and family [12]. Therefore, gatekeeper training enables participants to recognize linguistic, behavioral, and emotional warning signs and to evaluate suicide risk among people around them, equipping the former, as gatekeepers, to provide prompt assistance, primarily by referring the latter to mental health care institutions. Thus far, the primary target audience for gatekeeper training has been the public, particularly students. In Korea, the Suicide CARE 2.0 program (basic: 2 hours, condensed: 1 hour) has been widely implemented as a form of gatekeeper training. Suicide CARE provides three specific guidelines regarding gatekeeper intervention for people at high risk of suicide: “Careful observation” covers the detection of verbal and non-verbal signals for suicidal intents; “active listening” aims to actively hear the cause of suicidal intention; and “risk evaluation and expert referral” involve referring suicidal persons to mental health professionals [13,14].
Gatekeeper training can impact four common factors related to suicide: suicide knowledge, attitudes, self-efficacy, and preventive behavioral intentions. Specifically, suicide knowledge, self-efficacy, and preventive behavioral intentions are reported to be significantly improved at one month [15,16], three months [13,17,18], six months [19,2], and up to 12 months[21] after the gatekeeper training. However, the relation between suicide prevention attitudes and gatekeeper training is inconsistent, with some studies reporting the effects being retained up to three months after training [17] while others report no significant effects [16] or only partial effects on certain aspects of attitude [13]. In other words, suicide prevention attitudes may or may not be improved by gatekeeper training.
Nonetheless, the current findings suggest that gatekeeper training for families of PMDs may help families recognize suicide risk and provide support appropriately. However, despite evidence supporting the effectiveness of gatekeeper training, research on gatekeeper training and its effects have three major limitations. First, the study populations are primarily limited to the general population (e.g., students, teachers) [15-17,19,21], with no study investigating gatekeeper training tailored to the families of PMDs—a group with high suicide risk.
Second, most studies have not adopted a randomized controlled trial (RCT) design. Only a few studies are RCTs or cluster RCTs [13,21], and the majority of the studies have used a quasi-experimental design [15-20]. In other words, most existing studies are non-RCTs and thus have inadequate internal validity. This means that the observed effects cannot be directly attributed to the gatekeeper training, as unexpected confounders might have had untested influences.
Third, a substantial number of existing studies have performed only a short follow-up. A systematic review by Holmes et al. [22] revealed that the follow-up period for the effects of gatekeeper training for the public is generally between one and three months. While it is important to investigate the long-term effects of gatekeeper training, several practical limitations exist in measuring the pure effects of this training, especially for families of PMDs.
For example, many families of patients who utilize community psychiatric rehabilitation centers (CPRCs) in Korea participate in group education every one to two months, and a follow-up period of at least three months may lead to the effects of gatekeeper training being confounded with other types of education for families of PMDs. Additionally, withholding long-term education from the control group of families with mental disorders is ethically problematic. Therefore, short-term 1-month follow-ups may be an alternative for assessing the standalone effects of gatekeeper training while minimizing ethical concerns for families of PMDs.
In essence, there is a need for specialized gatekeeper training for families of PMDs, and the effectiveness of such training should be validated through RCTs with a follow-up period of at least one month, considering the educational conditions and special needs of the study population. In this context, the Korea Foundation for Suicide Prevention (KFSP) has developed the suicide prevention education program for families of people with mental disorders (SPEM-F) [11]. SPEM-F is a 1-session (90 minutes) program that provides face-to-face, offline training to group members. This includes the core elements of gatekeeper training and information on psychiatric symptoms and exercises for effective communication with PMD. Therefore, SPEM-F focuses on imparting suicide knowledge, improving attitudes, increasing self-efficacy, promoting preventive behavioral intentions, and enhancing communication skills.
While developed based on existing literature, SPEM-F has not been assessed for effectiveness. As the program is being considered for wider implementation in CPRCs in Korea, it is crucial to evaluate its effectiveness. Thus, we aimed to examine whether families who have completed SPEM-F show significantly better suicide knowledge, attitudes, self-efficacy, preventive behavioral intentions, and communication skills, compared with those who have not completed the program.
METHODS
Participants
We recruited 66 family members of PMDs who utilized a CPRC in Korea. The inclusion criteria were as follows: family member living with PMD (e.g., parent, child, spouse, sibling), adult aged 19 years and older, provision of informed consent to participate in the study, and no plans to take another suicide prevention education within three months before or after study participation. The exclusion criteria were people who were currently being treated for a psychiatrist’s diagnosis of schizophrenia and other psychotic disorders or bipolar and related disorders.
We determined the sample size as 44 using G*Power 3.1.9.7 (Franz Faul, Heinrich Heine University Düsseldorf, Düsseldorf, Germany). To enhance the external validity, we increased the target sample to 60, and to account for a 10% dropout rate, we enrolled 66 participants (33 in the experimental group, 33 in the control group). The conditions for calculating the sample size using G*Power were set as follows, with reference to previous studies [23,24]: repeated-measures analysis of variance (ANOVA) within–between interaction, effect size of 0.25, p-value of 0.05, power of 0.95, two groups, and three measurements.
The recruitment announcement involved sending participation letters to CPRCs nationwide, including 80 day rehabilitation centers, of which eight CPRCs (day rehabilitation centers: 7, other: 1) expressed their intention to participate. After we posted the recruitment announcement, 66 potential candidates volunteered (from eight CPRCs nationwide), but three withdrew during the recruitment announcement stage, and four withdrew during the baseline testing after enrollment. Thus, our analysis only included data from 59 participants (experimental group: 30 from 4 CPRCs; control group: 29 from 4 CPRCs) (Figure 1).
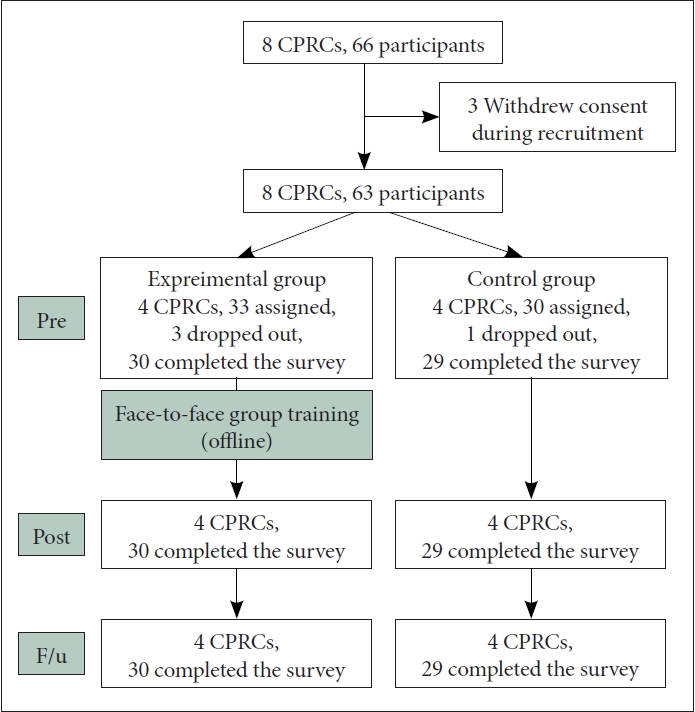
Flow chart of recruitment process of the study participants. CPRC, community psychiatric rehabilitation center; F/u, follow-up.
Study design
We analyzed the effects of SPEM-F through a cluster RCT. Given that the participants were from eight CPRCs dispersed nationwide (Seoul city: 2, Gyeonggi province: 1, Daegu city: 3, Busan city: 2), we first matched the size of the area (e.g., the metropolitan or local areas) and randomized the facilities. The experimental and control groups completed the same online questionnaire according to the designated time points. The outcome variables were suicide knowledge, attitude, self-efficacy, preventive behavioral intention, and communication, and these variables were measured based on the scales widely used in previous studies about gatekeeper training [13,24]. Three measurements were taken three days before training, immediately after training, and at a 1-month follow-up. The control group also completed the questionnaires at the same intervals. The pre- and post-training questionnaires contained items from five scales, but the order of the post-training items was changed randomly to prevent practice effects that may be caused by the short measurement intervals [25,26]. The order of the items was the same in the pre-training and follow-up questionnaires.
The experimental group completed SPEM-F after the pre-training survey. Participants in the control group were also given an opportunity to participate in the program after the completion of the follow-up survey. To ensure standardized lectures, we recruited three mental health professionals (social workers: 2, nurse: 1) with more than seven years of experience, as the instructors. We provided them with instructions for the standard lecture format for SPEM-F.
Measurements
Participation application and demographic questionnaire
This application was completed at the time of study participation. It contained information on the participant (name, sex, age, relationship with the member, participant’s own mental health problems) and the PMD they were providing care for (sex, age, time since onset, primary diagnosis, history of suicide attempt, length of facility use). Participation motivation was assessed with a single item rated on a 7-point scale, where a higher score indicated greater motivation.
Self-Evaluation of Knowledge
We assessed suicide-related knowledge using Self-Evaluation Knowledge (SEK) developed by Wyman et al. [21] and adapted by Ryu [27]. SEK comprises nine items, one of which (on “Question Persuade Refer” [28] item) was revised for our study (before revision: how to document appropriately; after revision: how to communicate appropriately to prevent suicide). Each item is rated on a 7-point scale, with higher scores indicating more positive self-evaluation of one’s knowledge about suicide prevention. The internal consistency (Cronbach’s α) was 0.97 in Wyman et al. [21 and Ryu [27], and 0.94 for pre-training, 0.96 for post-training, and 0.97 for follow-up in our study.
Attitude Toward Suicide-20
We assessed attitude toward suicide using Attitude Toward Suicide-20 (ATTS-20) developed by Renberg and Jacobsson [29] and adopted by Park and Kim [30]. ATTS-20 comprises 20 items, with each item rated on a 5-point Likert scale. A lower score indicates a more permissive attitude toward suicide and an attitude suggesting that suicide is a universal phenomenon that cannot be prevented or predicted. The internal consistency was 0.66 in Ji et al.’s study [31] and was 0.71 for pre-training, 0.66 for post-training, and 0.72 for follow-up in our study.
Preparedness to Help Scale
We assessed preparedness to help using Preparedness to Help Scale (PHS) developed by Baber and Bean [32] and modified by Industry-Academic Cooperation Foundation Kyung Hee University [24]. PHS comprises four items rated on a 5-point scale; a higher score indicates greater preparedness to help, that is, greater self-efficacy for intervention. The internal consistency was 0.85 in the study by Baber and Bean [32], 0.93 in the study by Industry-Academic Cooperation Foundation Kyung Hee University [24], and 0.83 for pre-training, 0.88 for post-training, and 0.84 for follow-up in our study.
Suicide Prevention Behavior
We assessed preventive behavioral intention using Suicide Prevention Behavior (SPB) developed by Wyman et al. [21] and adapted by Kim and Kim [33]. SPB comprises eight items rated on a 5-point Likert scale, with higher scores indicating a greater possibility of engaging in SPB. The internal consistency was 0.90 in the study by Kim and Kim [33] and 0.95 for pre-training, 0.89 for post-training, and 0.93 for follow-up in our study.
Family problem-solving communication
We assessed family problem-solving communication using an instrument developed by McCubbin et al. [34] and adapted by Lim and Han [35]. This 10-item instrument uses a 4-point Likert scale, with three reverse-scored items; a higher score indicates more positive problem-solving communication. The internal consistency was 0.89 in the study by McCubbin et al. [34], 0.85 in the study by Lim and Han [35], and 0.81 for pre-training, 0.82 for post-training, and 0.78 for follow-up in our study.
Programs
SPEM-F is a single-session (90 minutes), face-to-face offline group program, and the target audience includes families of PMDs. The aim of SPEM-F is to improve family members’ suicide knowledge, attitudes, self-efficacy, preventive behavioral intentions, and family communication skills. Accordingly, the program addresses understanding depressive symptoms, psychiatric disorders and suicide, suicide warning signs, family communication to prevent suicide, and evaluation and response to suicide risk (Table 1). The instructor qualifications for SPEM-F were psychiatrists and mental health professionals. SPEM-F was developed in December 2019 and was given preliminary accreditation as an in-person suicide prevention program by the Korean Ministry of Health and Welfare (MOHW) and KFSP in June 2020 [36].
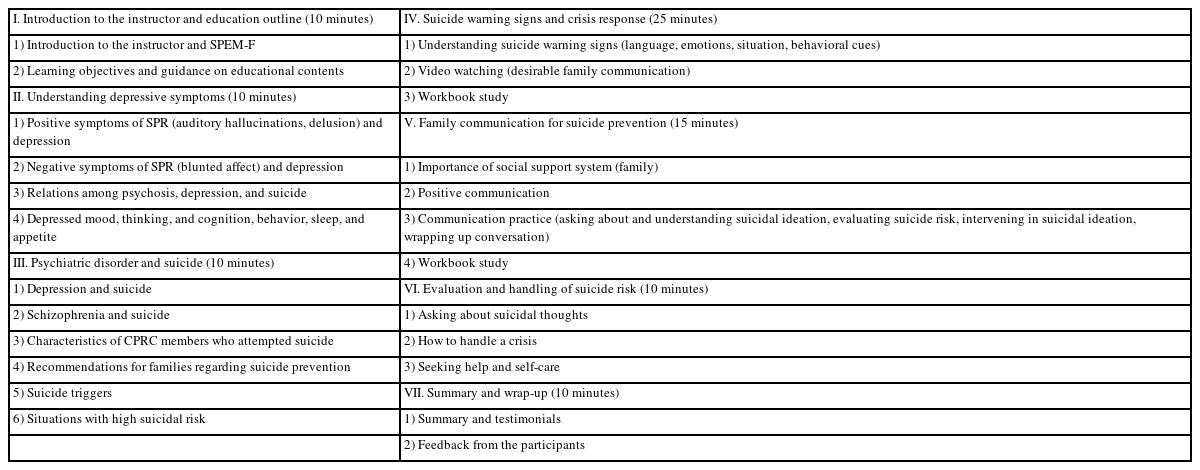
Introduction to SPEM-F (90 minutes)
Procedure
This study was conducted from May to December 2022 and was approved by the MOHW (IRB No. P01-202208-01-017). We explained the purpose and process of the study to the participants and obtained their informed written consent. We then sent an online questionnaire to individual participants three times at the designated time points, and the participants returned the completed questionnaires to us. To prevent participant dropouts, we sent text message reminders before and after the survey time points and collected the data with the cooperation of facility staff. We considered the following participants as dropouts: those who expressed the decision to stop participating in the study during the survey and those who did not complete one scale or more on the survey. A small gift was offered to participants who completed the survey at least once.
We used IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA), to analyze the collected data. Before conducting the analysis, we changed the order of the items in the post-education survey back to the original order. Statistical significance (α) was set to 0.05, and the reliability of the instruments was tested using the internal consistency coefficient. We performed cross-tab analyses (e.g., chi-squared test [χ2], Fisher’s exact test) and independent samples t-test to verify the baseline homogeneity of the two groups. We used repeated-measures ANOVA to examine significant differences in the dependent variable by time and group.
RESULTS
Demographic characteristics
Cross-tab analysis results showed that the demographic characteristics between the two groups were not significantly different (Table 2). These results suggested that the two groups were homogeneous in their demographic variables at baseline.
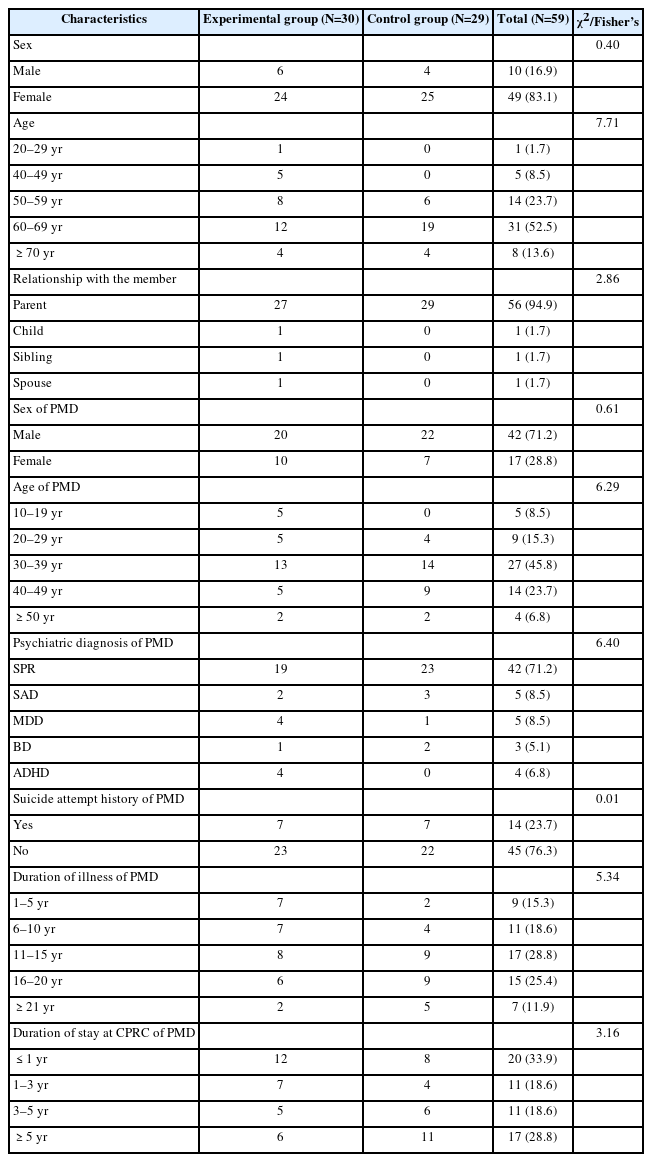
Demographic characteristics of the participants
Baseline homogeneity in participation motivation and dependent variables
Prior to investigating the effectiveness of the program, we performed independent t-tests on the homogeneity of the two groups in terms of participation motivation and dependent variables. The results showed that participation motivation (score range: 0–6) was high in experimental (mean [M]=3.97) and control groups (M=4.72), with no significant difference between them (t(57)=-1.86, not significant [n.s.]). We also found no significant differences in the baseline scores for the dependent variables between the two groups (Table 3): suicide knowledge, t(57)=-1.89, n.s.; attitude, t(57)=-0.39, n.s.; self-efficacy, t(57)=-0.95, n.s.; preventive behavioral intention, t(57)=-1.07, n.s.; and communication, t(57)=-1.97, n.s. These results confirmed that the two groups were homogeneous in their participation motivation and dependent variables at baseline.

ANOVA results on the effectiveness of SPEM-F
Validation of SPEM-F
We analyzed the effectiveness of SPEM-F with repeated-measures ANOVA, including interaction effects. The experimental group showed a significant improvement in suicide-related knowledge, self-efficacy, and preventive behavioral intention compared with the control group, including increased family problem-solving communication. Moreover, these effects were maintained for at least one month.
As shown in Table 3 and Figure 2, suicide knowledge had a significant group and time interaction effect (p<0.001). In the experimental group, suicide knowledge increase was higher at the post-training (M=29.50) than pre-training (M=18.13) measure, and although it slightly decreased to 24.83 at the 1-month follow-up, it was still higher than that at the pre-training measurement (M=18.13). In the control group, suicide knowledge showed a consistent downtrend across the pre-training (M=23.83), post-training (M=22.03), and 1-month follow-up (M=20.34) measurements.
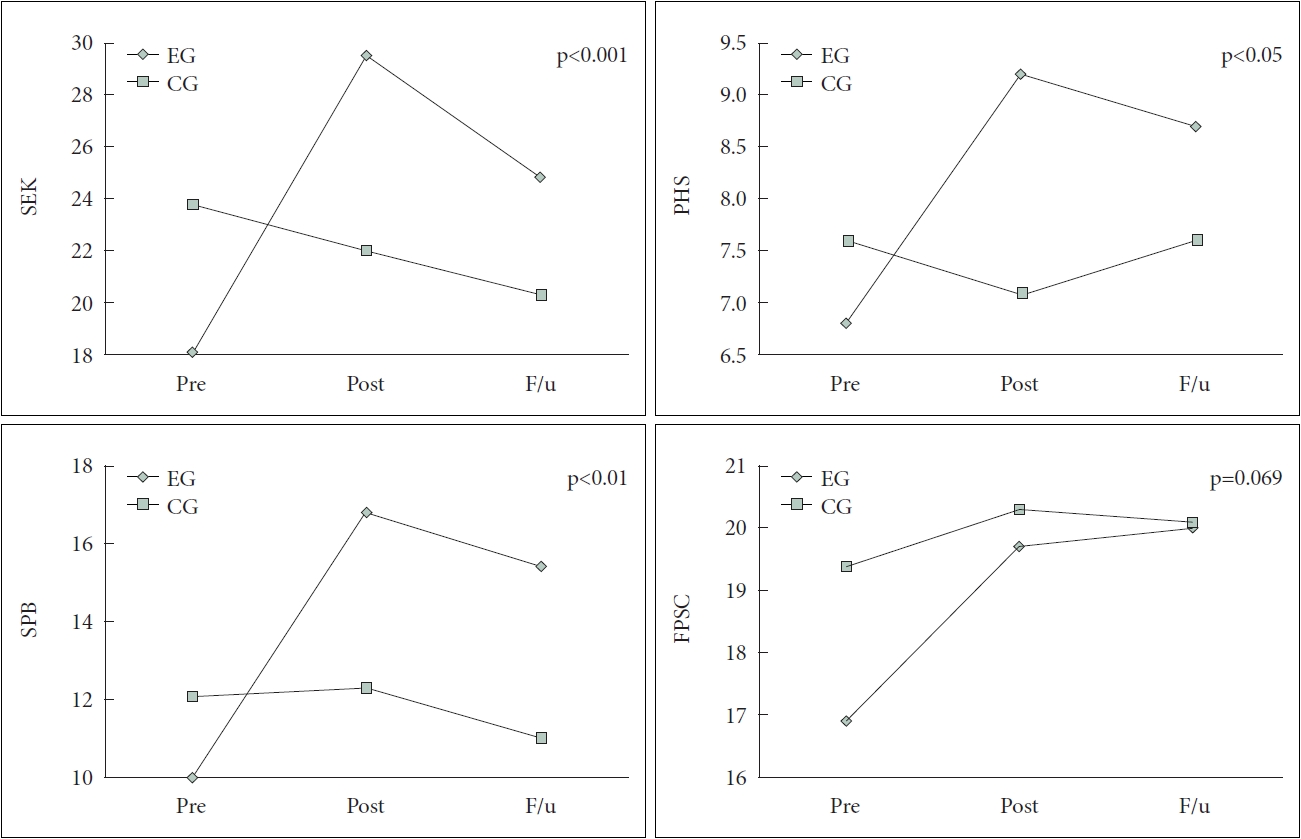
Group and time interaction effects of the dependent variables. SEK, self-evaluation of knowledge in suicide prevention; PHS, preparedness to help; SPB, suicide prevention behavior; FPSC, family problem-solving communication; EG, experimental group; CG, control group; F/u, follow-up.
We found no significant group and time interaction effect on attitude toward suicide. An additional analysis of the items revealed that the experimental group showed positive attitude changes regarding the perception of suicide (e.g., People who make threats seldom complete suicide; Can always help) and decision process (e.g., Suicides considered for a long time; Suicide decision cannot be reversed) compared with the control group.
Meanwhile, we noted a significant group and time interaction effect for self-efficacy (p<0.05). In the experimental group, self-efficacy was higher at the post-training (M=9.20) than pre-training (M=6.87) measure, and although it slightly decreased to 8.73 at the 1-month follow-up, it was still higher than that at the pre-training (M=6.87) measurement. In contrast, the control group did not show significant changes in their self-efficacy scores across the pre-training (M=7.66), post-training (M=7.14), and 1-month follow-up (M=7.66) measurements.
Preventive behavioral intention likewise showed a significant group and time interaction effect (p<0.01). In the experimental group, preventive behavioral intention was higher at the post-training (M=16.83) than pre-training (M=10.07) measure, and although it slightly decreased to 15.43 at the 1-month follow-up, it was still higher than that at the pre-training (M=10.07) measurement. In contrast, the control group did not show significant changes in their preventive behavioral intention scores across the pre-training (M=12.14), post-training (M=12.34), and 1-month follow-up (M=11.07) measurements.
Finally, we observed a trend of group and time interaction for family problem-solving communication (p=0.069). The experimental group showed a consistently rising trend in communication from pre-training (M=16.97) to post-training (M=19.70) and 1-month follow-up (M=20.07) measures. However, the control group did not show significant changes in their communication scores across the pre-training (M=19.45), post-training (M=20.31), and 1-month follow-up (M=20.14) measurements.
DISCUSSION
We examined the effects of gatekeeper training for families of people with schizophrenia and other mental disorders, based on SPEM-F. Our study’s experimental and control groups showed no significant differences in their baseline demographic characteristics. Moreover, among PMDs in our study, 47 individuals (79.7%) had schizophrenia or schizoaffective disorder, 14 individuals (23.7%) had made at least one suicide attempt, and 50 individuals (84.7%) received the diagnosis six or more years ago. In addition, 41 individuals (69.5%) fell within the age range of 30 to 49 years, while 39 individuals (66.0%) had a duration of stay at CPRCs for one year or more.
This finding coincides with previous reports on the high rate of suicide attempts among PMDs and the prevalence of schizophrenia among PMDs who utilize CPRCs in Korea [5-8]. Families of middle-aged adults with mental disorders are exposed to extended periods of caregiving duties. Hence, while the role of gatekeeping is essential for preventing suicide among PMDs, gatekeeper training must address the caregiver stress and prevention of burnout for families of PMDs.
We found that gatekeeper training tailored to families of PMDs was generally effective. Suicide-related knowledge, self-efficacy, and preventive behavioral intention improved immediately after the training and retained up to the 1-month follow-up. This suggests that families of PMDs acquire knowledge and resources to respond to suicidal crises and increase their confidence or self-efficacy to react to warning signs among PMDs after the gatekeeper training. Furthermore, problem-solving communication within families showed an increasing trend immediately and up to one month after the gatekeeper training.
These results are consistent with previous findings that gatekeeper training can substantially improve the knowledge, self-efficacy, and preventive behavioral intentions necessary for recognizing and referring people at risk of suicide as well as boosting their confidence in intervening in the situation, thereby increasing their likelihood of taking action to help suicidal individuals [22]. Moreover, our findings suggested that SPEM-F encompasses not only the basic elements of gatekeeper training but also communication practices based on understanding psychiatric symptoms. Existing gatekeeper programs have mainly focused on the general population, often neglecting the role of family members. Consequently, people who have a close relationship with those at risk of suicide have had difficulty applying the training in real-life situations [37]. Our findings confirmed that SPEM-F may be implemented among families of PMDs who are at risk of suicide.
Participants’ attitudes toward suicide prevention did not improve immediately after the training and up to one month of follow-up. However, further analysis of the questionnaire items revealed changes in some aspects of attitudes pertaining to the perception of suicide and process of suicide decision. One possible explanation for these findings may lie in the fact that existing programs have not placed sufficient emphasis on attitude change through focused training, despite their benefits in improving knowledge, self-efficacy, and preventive behavioral intentions [22,37]. Short training sessions (e.g., 1–2 hours) may not be adequate to induce significant attitude change among participants, and insufficient attitude change may ultimately undermine the sustainability of the effects of gatekeeper training. Given that attitude change is a key factor in promoting sustained behavioral change, future studies may need to adjust the structure and duration of the program to accommodate a broader range of age groups and assess the retention of the benefits of training, including changes in attitude toward suicide.
The clinical implications of this study are as follows: First, we verified the effectiveness of SPEM-F and confirmed the need to expand its implementation. Specifically, families of PMDs who participated in SPEM-F were found to have gained knowledge on assisting people at risk of suicide, contacting relevant organizations, and recognizing suicide warning signs, as well as awareness for suicide. These findings suggest that repeatedly providing SPEM-F as gatekeeper training to families of PMDs at CRPCs would enable families to gain a deeper understanding of the relation between mental disorders and suicide and become more interested in gatekeeping activities.
Additionally, our results highlighted the need for refresher or advanced gatekeeper suicide prevention education programs. Although we successfully validated the effectiveness and utility of SPEM-F, the one-time nature of the program (90 minutes) may not be sufficient to facilitate gatekeeper activities by families of PMDs who are at high risk of suicide. Moreover, the program was not effective in improving the participants’ attitudes toward suicide, which highlights the need for a refresher or advanced gatekeeper training even if not specifically tailored to the families of PMDs.
At present, dozens of MOHW- and KFSP-certified suicide prevention education programs are already available in Korea [36]. Although developed with different objectives and purposes, these programs overlap considerably in their contents owing to the nature of the education. Moving forward, it is imperative to conduct an integrated analysis of existing suicide prevention education programs to identify common and distinct factors among them, and to develop a comprehensive plan for the development of novel programs.
Our study has some limitations. First, SPEM-F was developed to address the general gatekeeper educational contents and the characteristics of people with severe mental disorders. Therefore, the observed educational effects may be attributed to the program’s tailoring to this group or to the general content of suicide prevention education. Future studies should evaluate the effects of a suicide prevention education program designed for the general population (e.g., Suicide CARE 2.0) on families of PMDs.
Second, most participants were older adults caring for long-term schizophrenic patients. Consequently, the findings may not be generalizable to caregivers of people with different mental disorders, various disease stages, or differing age groups. Future research should involve a more diverse sample to enhance generalizability.
Third, although we limited the follow-up period to one month under practical and ethical considerations, long-term follow-up may be possible in research facilities other than CPRCs. Subsequent studies should perform more extended follow-ups of six months or longer for various groups to identify the appropriate timing of second or refresher gatekeeper training [22]. Most of all, it is crucial to devise an appropriate analytical approach that enables the measurement of the sole effect of SPEM-F over an extended follow-up period.
Fourth, the ultimate goal of suicide prevention education is to contribute to reduced suicide rates. We measured preventive behavioral intention as one of the dependent variables, and future studies with long-term follow-ups should also measure the frequency of gatekeepers identifying, intervening, and properly referring at-risk people to relevant resources. As their gatekeeper activities are the final outcomes of their personal inclinations and training received, the psychological characteristics of gatekeepers suitable for training and activities should also be elucidated.
In conclusion, our findings showed that SPEM-F is an effective evidence-based gatekeeper training program for families of PMDs. To prevent suicide among PMDs and their families, this training program should be adopted by many mental health institutes in the future.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Deuk-Kweon You, Jeoung-Mo Son. Data curation: Deuk-Kweon You, Jeoung-Mo Son. Formal analysis: Deuk-Kweon You. Investigation: Deuk-Kweon You, Jeoung-Mo Son. Methodology: Deuk-Kweon You. Project administration: Tae-Yeon Hwang. Supervision: Tae-Yeon Hwang. Writing—original draft: Deuk-Kweon You. Writing—review & editing: Deuk-Kweon You, Tae-Yeon Hwang.
Funding Statement
This research was supported by a fund (project no. 2022-03) for a research of the Korea Foundation for Suicide Prevention.
Acknowledgements
We thank Yoon-Ah Lee and Min-Ji Yu at the Korea Foundation for Suicide Prevention for helping with data collection.