INTRODUCTION
Depression is very common among the elderly and is one of the major geriatric psychiatric disorders and a critical risk factor for mortality and disability [1]. The World Health Organization estimated that the prevalence of depression in the elderly is between 10% and 20% worldwide [2]. Depression in older adults results in significant loss of skills accelerates the progress of physical illnesses, increases deaths from suicide and physical diseases, and thus causes high consumption of health care services [3]. Additionally, it leads to a lack of social connection, poor self-care, poor quality of life, and the occurrence of various diseases [4].
Depression in the elderly differs from general adult depression in both subtle and obvious ways. Symptoms, etiology, risk and protective factors, and potential prognoses all have their own characteristics throughout life. First, the elderly are exposed to various physical illnesses. Diabetes, dementia, stroke, Parkinson’s, infections, and thyroid conditions have been identified as biological risk factors for aging adults with depression. Second, there are characteristic psychosocial factors in the elderly, such as social isolation, loneliness [5], lack of exercise or physical activities [6], and functional limitations in daily activities [7]. Third, depression in the elderly tends to be underdiagnosed and undertreated [8]. Depressive mood, loss of interest, and changes in personality are considered a natural part of aging. Also, depression in older adults may present somewhat differently than in younger adults. For example, older adults are less likely to endorse cognitive-affective symptoms of depression, including dysphoria and worthlessness/guilt, than younger adults [9]. Therefore, the elderly are less likely to detect depression or visit hospitals than young people, related to the poor prognosis of depression in the elderly. Additionally, there are two possible factors related to the poor prognosis of elderly depression [10]. Firstly, late-onset depression is associated with a high rate of hyperintensities in the brain on magnetic resonance imaging, which is related to cerebrovascular diseases. There is evidence that these findings predict a worse recovery from depression in the elderly [11]. Secondly, the physical illness and disability of the elderly limit their daily activities, which becomes an obstacle to the recovery of individuals with depression [12]. The major cause of this difference is aging. Aging is a complex process of various physical and psychological changes, resulting in gradual losses that result in an individual being less adapted to their environment. These elderly people who negatively separate aging from daily lives or social relationships are likely to experience more negative emotions. One of the negative emotions that often occur in the elderly is helplessness [13]. This is related to the feelings of failure that occur more in older age than in younger age.
Depression often occurs in relation to cognitive impairment [14]. Although there are various estimates, studies have shown that about 25% of the elderly have a combination of depression and cognitive dysfunction [15]. The prevalence of depression in MCI patients is known to range from 16.9%-55% [16]. Late-life depression is associated with a two-fold increased risk of dementia [13] and is clinically associated with an increased risk of dementia and Alzheimer’s disease [17]. Several studies report a link between depressive symptoms in participants with MCI and later progression to dementia. Even mild depressive symptoms were identified as important factors related to poorer function and quality of life in MCI patients [18]. Treatment of depression in the elderly with cognitive impairment at an appropriate time is also very important in terms of the patient’s prognosis, level of function, and ultimately quality of life. The coexistence of cognitive impairment and depression has been related to an increase in mortality, a decrease in quality of life, and an increase in the burden and pain of caregivers. Due to the negative impacts on caregivers, the coexistence of depression and cognitive impairment is associated with a higher rate of institutionalization in dementia patients [19]. Hospitalized dementia patients are exposed to various medical complications, including mental stress and hospital-acquired infection, which reduce their quality of life and exacerbate cognitive decline. Since depressive symptoms in the cognitively declined elderly are caused by a variety of complex factors and have important implications for the later prognosis, it is important to understand the pattern of depressive symptoms in this population, which means that providing appropriate outside help, such as interpersonal therapy or other supportive cares, in addition to medication, is critical to the treatment and management plan for them.
Network analysis is a new modeling method that has been used to explore the interconnected symptom structure of mental disorders [20]. This approach can propose novel methods for analyzing data, modeling, and simulating psychopathological processes in different ways [21]. This network perspective assumes that the symptoms reinforce each other to maintain the disorder and that these patterns characterize the disorder. The network approach has the advantage of emphasizing the locational importance of symptoms within a disease [22], quantifying the importance of symptoms (nodes) as explained by their centrality in the network, which enables us to construct a larger picture of how symptoms are associated with each other. Several network analyses have been performed on a variety of mental disorders, such as depression, post-traumatic stress disorder, psychotic disorders, substance abuse, and so on [21]. In relation to depression, several studies have shown that previous negative emotions have a greater effect on the next emotional states, making individuals experiencing negative emotions more resistant to the treatment of depression [23]. Other studies have revealed associations between losing loved ones and depressive symptoms. Specifically, it has been found that “loneliness” activates other depressive symptoms through its association with loss and connects to other risk factors such as lack of instrumental social support [24]. However, to our knowledge, a network analysis of depressive symptoms coexisting with MCI and early stage dementia has not yet been conducted so far. We determined that network analysis could be employed as a useful measure to reveal the mechanism underlying depression in patients with MCI and early stage dementia. Therefore, the purpose of this study is to investigate the characteristics of depression symptoms in the elderly with cognitive impairment through this network analysis technique. This study aimed to estimate the network structure of depression in patients with MCI and early stage dementia by setting subscales of Korean form of Geriatric Depression Scale (KGDS) to each node to perform network analysis, and then specifically analyze which symptoms of depression are the most central and which have the greatest correlation with each other.
METHODS
Participants
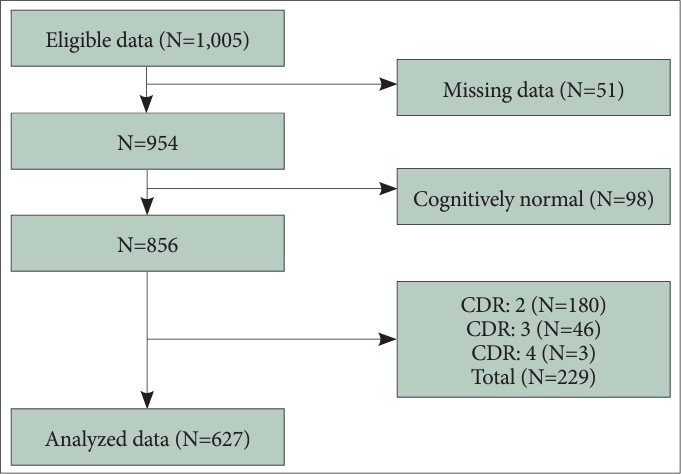
Among patients who visited the dementia clinic for memory complaints at Konkuk University Medical Center from June 1, 2020 to December 31, 2021, patients aged 60 or older who were diagnosed with mild cognitive impairment (MCI) or dementia were included. MCI and dementia were diagnosed according to the diagnostic criteria for mild neurocognitive disorder and major neurocognitive disorder of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Of the initial 1,005 registered patients, 51 were excluded due to missing data and 98 additional patients with normal cognitive function were excluded. Furthermore, for reliable responses to self-reported questionnaires, patients that measured a 2 or higher Clinical Dementia Rating (CDR) score were excluded. Accordingly, a total of 627 patients were included in the analysis (Figure 1). This study was approved by the Institutional Review Board (IRB) of Konkuk University Medical Center. Due to the retrospective nature of the study, the informed consent has been waived (IRB No. KUMC 2023-04-019).
Measures
Expanded Clinical Dementia Rating scale
The CDR is a global rating measure for patients diagnosed with dementia, which can be staged as normal, questionable, mild, moderate, or severe [25]. CDR consists of a semi-structured interview of the subject and the reliable informant based on the clinical judgment of the clinician. It is calculated by testing three cognitive domains (memory, orientation, judgment, and problem-solving) and three behavioral domains (community affairs, home and hobbies, and personal care) [26]. The Korean version of the CDR was used in this study [27]. The expanded CDR is based on a scale of 0-6: none (CDR=0); questionable (CDR=0.5); 1=mild; 2=moderate; 3=severe; 4=profound, and 5=terminal.
Global Deterioration Scale
The Global Deterioration Scale (GDS) provides caregivers with an overview of cognitive functional stages for those suffering from primary degenerative dementia [28]. It is divided into 7 different stages. Stages 1-3 are the pre-dementia stages. stages 4-7 are the dementia stages. From stage 5, an individual can no longer survive without assistance. Within the GDS, each stage is numbered (1-7), given a short title (i.e., forgetfulness, early confusion, etc.), and followed by a brief listing of the characteristics of that stage. A Korean form of GDS (KGDS) was translated and validated, and the reported internal consistency was 0.88 [29].
KGDS
The Geriatric Depression Scale (GDS) [30] is widely used in clinical and research settings to assess depression in older adults. The GDS comprises 30 questions that evaluate the participant’s mood in the preceding week. The participants choose the responses “yes” or “no,” with “yes” counted as 1 and “no” counted as 0 to yield a range of total scores from 0 to 30. As the score increases, individuals experience more depressive symptoms. A score of 14 is the cut-off point for the diagnosis of depression. A Korean version of GDS was translated and validated, and the reported internal consistency was 0.88 [31].
Statistical analysis
Analyses for descriptive statistics were performed using the Statistical Package for the Social Sciences, version 17 (SPSS Inc., Chicago, IL, USA) with significance established at p<0.05. Network analyses were conducted using “IsingFit” and “qgraph” packages in R [32]. Because the scores for each item were binary, Isingfit package was used to fit the data [33]. IsingFit package uses the “elasso” method, where: a logistic regression is produced from the variables (i.e., a variable is regressed onto all other variables) and a penalty is imposed on the regression coefficients to get close to the true network. IsingFit employs Extended Bayesian Information Criterion for the parsimonious selection of network solutions with fewer neighboring nodes. Very small coefficients are also set to zero. The network contained 30 nodes corresponding to the subscales of the KGDS. The network was constructed using the 30 nodes at each point and was graphically illustrated using the “qgraph” package [32], which implemented the Fruchterman-Reingold algorithm to place connected nodes closer [34].
Next, network centrality (strength, betweenness, and closeness) was calculated to determine whether a certain item was more or less relevant to other items. The node strength of a focal node is defined as the sum of all connections to adjacent nodes. A high node strength indicates a strong connection to the connected nodes. A symptom with high strength has a strong association with symptoms that appear in adjacent nodes. Betweenness indicates the importance of focal nodes in the shortest path between different node pairs [35]. At a high betweenness, it can be expected that the symptom will appear more frequently in the connecting path between other symptoms. Finally, closeness indicates how close the focal node is to other nodes. Closeness is computed by measuring the average distance from the focal node to other nodes. The high closeness of a node means that its changes may quickly affect other nodes in the network [36]. A symptom with high closeness can be seen as a good predictor of other symptoms.
The reliability and interpretability of the estimated networks were determined using the bootnet R-package. Correlation stability coefficients is an index indicating the stability of centrality indices, and less than 0.25 is not interpreted as having poor accuracy [37]. Finally, we determine edge weight accuracy using a nonparametric bootstrap method with 1,000 bootstrap samples, which provides information on whether a particular edge is significantly different from others.
RESULTS
Descriptive statistics
Of the 627 participants, 36.7% were male and 63.3% were female. Subjects’ ages ranged from 60 to 98, with a mean age of 76.20 and a standard deviation of 7.71. The mean KGDS was 13.12±7.26. Table 1 indicates participant demographics and the frequency of their responses for CDR, GDS, and KGDS.
Network estimation and centrality
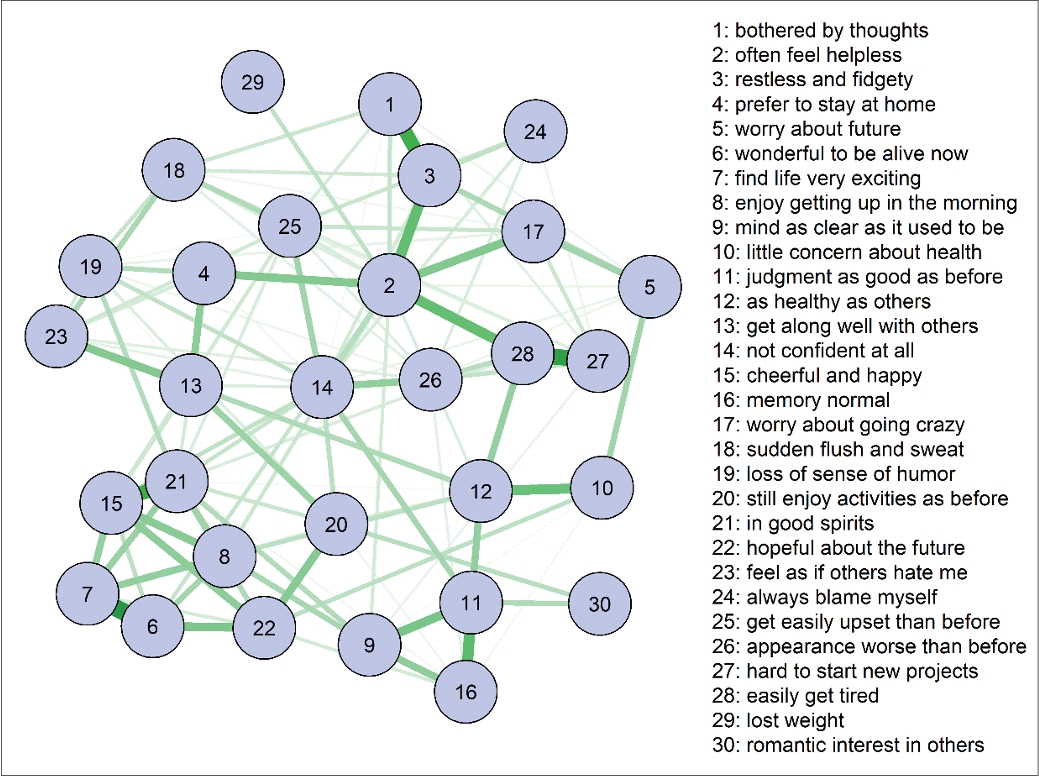
The estimated network is demonstrated in Figure 2. Figure 3 shows the centrality indices for strength, betweenness, and closeness for each node. The correlation stability coefficients for strength and betweenness were 0.516 and 0.284, respectively. Therefore, these results are considered stable and subsequently interpreted [37]. Since the closeness coefficient was 0, which is less than 0.25, it is too unstable to be interpreted. Figure 3 demonstrates high node strengths of KGDS 2 (often feel helpless), KGDS 21 (in good spirits), KGDS 14 (not confident at all), and KGDS 15 (cheerful and happy), showing that these nodes are strongly connected to their adjacent nodes. In contrast, only KGDS 2 (often feel helpless) had the highest node betweenness, indicating that it is expected to be more frequent in paths connecting one node to another.
Edge-weights bootstrapping
A non-parametric bootstrap method was applied to estimate a 95% confidence interval for each edge (Supplementary Figure 1 in the online-only Data Supplement). Confidence intervals for most edges overlap, but the first 9 edges are significantly stronger than others: the edges connecting KGDS 6 (wonderful to be alive now) and KGDS 7 (find life very exciting); KGDS 27 (hard to start new projects) and KGDS 28 (easily get tired); KGDS 15 (cheerful and happy) and KGDS 21 (in good spirits); KGDS 1 (bothered by thoughts) and KGDS 3 (restless and fidgety); KGDS 11 (judgment as good as before) and KGDS 16 (memory normal); KGDS 2 (often feel helpless) and KGDS 3; KGDS 2 and KGDS 28; KGDS 10 (little concern about health) and KGDS 12 (as healthy as others); and KGDS 9 (mind as clear as it used to be) and KGDS 11. The edge weights of edges connected to node KGDS 2 are demonstrated in Table 2. KGDS 3 and KGDS 28 showed the highest intensity of relationship with KGDS 2. This can also be seen in Figure 2, where edges connecting nodes 2 and 3, and 2 and 28 are the thickest and darkest.
DISCUSSION
The findings of this study suggest that helplessness was the most central symptom in depressive patients with MCI and early stage dementia. Of all items in KGDS, helplessness showed the highest strength and betweenness. Among other items, KGDS 21 (in good spirits), KGDS 14 (not confident at all), and KGDS 15 (cheerful and happy) also had high strength centralities, but they did not show high node betweenness. Another major finding from the network analysis was that helplessness showed the thickest and darkest edges with KGDS 3 (restless and fidgety) and KGDS 28 (gets tired easily).
Helplessness is a psychological state in which an individual who cannot exercise reasonable control in one situation considers themselves unable to exercise proper control in another [38]. Helplessness is known as one of the important mechanisms of depression. It is caused by repeated failure or frustration, which reduces an individual’s self-efficacy and self-esteem, eventually leading to depression. In fact, cognitive behavioral therapy for depression also puts helplessness as an important target. The elderly are thought to be particularly vulnerable to helplessness. It can be said that this is related to the sense of failure that occurs more in older age than in youth [39]. Not only when the elderly have a specific disease, but also in the normal aging process, cognitive ability gradually weakens and function decreases over time. Additionally, the elderly not only become physically weak as they age but also become more socially and economically vulnerable. The physical and mental frailties observed in the elderly often lead to a significant loss of confidence. This is evidenced by the high scores on the KGDS 14 scale, indicating a lack of confidence in our sample. We hypothesize that cognitive impairment may further contribute to a state of learned helplessness [40]. This is supported by the prevalence of depression in the early stages of dementia.
In our study, it was also found that helplessness plays the most central role of depressive symptoms in the elderly with MCI. Here, elderly patients with Alzheimer’s disease or other dementia are known to be more vulnerable to this sense of helplessness. Unlike dementia, patients with MCI can live a relatively independent daily life, but their overall cognitive functions such as memory, language ability, and attention-focus are deteriorated compared to others of the same age and educational background. The elderly with MCI experience a sense of helplessness generated by a decrease in physical function, interpersonal relationships, and psychological maladjustment due to aging [39]. Our study showed that helplessness is the most central symptom of depression in this group by including elderly people with MCI as well as early dementia. In a study comparing the results of network analyses of the elderly with cognitive impairment with those of healthy individuals, emotion-related items, such as “Do you feel depressed and discouraged?”, that did not appear as major depressive symptoms in the cognitively impaired group yielded major symptoms in the healthy group [41]. These results suggest that patients with cognitive impairment tend to undervalue their emotional symptoms and have difficulty consistently self-reporting their condition, making it difficult to assess emotional problems. This is consistent with our study, where helplessness was the primary symptom. This is also closely linked to the therapeutic meaning. It is suggested that helplessness can be the main treatment target for depression in patients with MCI because it is very central in the network of depressive symptoms. Improving autonomy, independence, and self-efficacy by providing appropriate external help in establishing treatment and management plans for elderly people with MCI is expected to play a positive role in preventing other symptoms of depression from worsening. A study of psychoeducation, cognitive rehabilitation, and cognitive-behavioral therapy for people with MCI found that these interventions helped patients better cope with an uncertain future by making them more accepting of their condition overall, and reduced perceptions of helplessness [42].
Another major finding from the network analysis was that helplessness and KGDS 3 (restless and fidgety), and KGDS 28 (gets tired easily) showed the thickest and darkest edges. The thickness and intensity of the edges mean that there is a very high correlation between the nodes they connect to. In other words, it can be seen that the relationship between helplessness and the two symptoms mentioned above is particularly stronger than other depressive symptoms. Fatigue is a condition described by a state of tiredness that does not resolve with rest or sleep, and it is one of the most common symptoms of depression in the elderly. Additionally, fatigue in the elderly can be caused by medical conditions, such as heart disease, cancer, chronic lung disease, or various other diseases. Therefore, fatigue is an important indicator of aging-related health and functional decline [43]. Fatigue causes the elderly to lose function in their various daily lives, which leads them to believe that they cannot do anything on their own. They believe that the outcome they want will be very unlikely or unfavorable, and depression occurs when they fall into the idea that no effort can change the outcome. This is also a model theory for the occurrence of learned helplessness, which is the main pathophysiology of depression [44]. In this study, helplessness, as a central symptom, was found to have a strong influence on other depressive symptoms. On the contrary, as described above, fatigue may affect the occurrence of helplessness among the elderly with depression. It can be seen that fatigue and helplessness have a two-way relationship that mutually affects each other.
Agitated depression includes symptoms such as restlessness (fidgetiness) or anger rather than sadness or despair which are usually typical of depressive symptoms [45]. Older adults are more susceptible to agitation as a component of depression [46]. Compared to younger patients, the elderly often exhibit more somatic symptoms of depression (i.e., sleep problems and abdominal pain), rather than emotional complaints such as self-criticism, guilt, failure, and sadness [47]. Consistent with these data, a meta-analysis shows that older adults with depression tend to experience more psychomotor agitation, restlessness, fidgeting, hypochondriasis, and general somatic symptoms compared to younger patients [48]. Additionally, agitation is one of the neuropsychiatric symptoms of dementia. One study shows that depression is the most common cause of dementia patients complaining of agitation [49]. Persistent agitation can develop a helpless cognition in an individual. Those individuals experience themselves as out of control, and they sometimes become disorganized in their daily lives. When this experience is repeated, patients are forced to feel helpless about their physical and psychological status [50]. Conversely, helpless rumination can also make an individual agitated, therefore, helplessness and agitation can be seen as mutually influential symptoms. In this context, it can be assumed that such cognitive distortion may occur more frequently in patients with MCI, due to their poor cognitive flexibility and impaired daily life function. Likewise, helpless rumination can also make an individual agitated.
Taken together, we believe that helplessness in depressive patients with MCI is mainly associated with physical symptoms such as anxiety and fatigue, which can be an axis of explaining the physical symptoms of senile depression. Conversely, when a patient with MCI visits the hospital complaining of the above physical symptoms of depression, it can be inferred that the central factor underlying these must be helplessness. Helplessness is the result of a combination of problems such as a decreased psychosocial function of the elderly, dissatisfaction in interpersonal relationships, and decreased self-efficacy, suggesting that depression treatment in the elderly with MCI requires interpersonal treatment or other auxiliary management in addition to medication treatment. In addition, depressive symptoms of the elderly with cognitive impairment are often physical, such as helplessness, fatigue, and agitation, and they may not adequately report their emotional difficulties. Therefore, it is important to closely monitor for symptoms of depression that may be underestimated in the elderly with cognitive impairment.
There are several limitations to this study. Firstly, this study was conducted in a cross-sectional way. The primary limitation of cross-sectional studies is that the temporal link between the outcome and the exposure cannot be determined because both are examined at the same time. Secondly, this study was conducted on patients with cognitive impairment, not the depressive patient group. Since the purpose of this study is to examine the characteristics of depressive symptoms in patients with cognitive impairment, more accurate results can be obtained when targeting patients with cognitive decline accompanied by depression. Thirdly, this study used self-report questionnaires to evaluate depressive symptoms. There are some biases such as recall bias and social desirability bias. Subjects may give the more socially acceptable answer rather than being truthful. Also, the subjects may not be able to assess themselves accurately.