INTRODUCTION
Irritability is a prevalent emotional state experienced by individuals, characterized by emotions such as anger, frustration, and discouragement, even in response to minor provocations, which can manifest as behavioral expressions such as anger outbursts [1-4]. It often includes a sense of difficulty in regulating rational emotions and can lead to verbal or behavioral explosions of anger [3,5]. Irritability can range from universal and non-pathological mood states to clear signs of mental disorders, presenting with varying degrees of severity and persistence. It is generally encountered in both psychiatric and nonpsychiatric medical settings [6-8]. For example, at least 40%-50% of adults with depression experience irritability, which is associated with the chronicity of depression, suicide risk, and impaired quality of life [9-11]. Irritability is often reported in anxiety disorders, such as generalized anxiety disorder, panic disorder, and social phobia [10]. Additionally, it is strongly related to impulsivity, and frequently observed in disorders characterized by difficulties in impulse control [12-14]. Moreover, irritability may act as a prognostic indicator for overall clinical responsiveness to specific medications [15]. Thus, developing an accurate definition and effective means of measuring irritability is imperative for advancing understanding and treatment.
Despite the prevalence of irritability in individuals with psychiatric disorders, precise measurement tools are lacking. Existing methods often rely on single-item questions incorporated within broader constructs, such as those found in the Beck Depression Inventory (BDI) and Young Mania Rating Scale. Recently, Craig et al. [2] developed the Irritability Questionnaire consisting of 21 items, and Stringaris et al. [4] developed parent and self-report scales with 7 items to assess irritability in children and adolescents. However, these scales have certain limitations. First, they are inefficient in solely assessing irritability as they measure it as part of other constructs. Second, their applicability is limited to specific populations, rendering them inadequate for assessing irritability across the full range of spectrum of individuals with psychiatric disorders. Finally, these scales involve a substantial number of items, making them impractical for quick symptom assessment in a clinical setting. Therefore, a tool is required that can measure a single construct of irritability in patients with psychiatric disorders using a minimal number of items while providing a rapid and accurate assessment in clinical practice. The Brief Irritability Test (BITe) developed by Holtzman et al. [16] in 2015 met these criteria. The original scale, initially comprising over 60 items, was condensed to a single-factor consists of only 5 items. This scale validated to assess irritability reliably and concisely among diverse samples, including over 1,000 undergraduate students and outpatients with chronic pain.
The objective of this study was to verify the validity and establish the reliability of the Korean version of the BITe for quickly and accurately measuring irritability, particularly among psychiatric patients.
METHODS
Study population
This study used data from self-report scales collected from 316 outpatients and inpatients who visited the Department of Psychiatry at Hanyang University Guri Hospital between July 2020 and March 2023. The inclusion criteria for participation were as follows: 1) had a current diagnosed psychiatric patient according to the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)-Clinician Version [17], 2) aged between 18 and 65 years, and 3) capable of reading and writing. More than 1/4 missing items or exhibiting random responses, such as consistently selecting the same response for all items, were excluded from the analysis because of the difficulty of interpreting the test results and the limited reliability of such data. Following adherence to the specified inclusion and exclusion criteria, 20 participants were excluded, resulting in the utilization of a total of 296 data points for the analysis. The study design was approved by the Institutional Review Board of the Hanyang University Guri Hospital (IRB no. 2022-03-034-002). Since the data was collected retrospectively from medical records, the requirement for patient informed consent was waived.
Measurements
BITe
This scale, developed by Holtzman et al. [16], consists of 5 items and uses a 6-point Likert scale ranging from 1 to 6. Higher scores indicate higher irritability. The internal consistency (Cronbach’s α) in this study was 0.89.
Barratt Impulsiveness Scale-11 (BIS-11)
A scale developed by Patton et al. [18] was used, which was validated by Heo et al. [19]. It consists of 30 items rated on a 4-point Likert scale ranging from 1 to 4, and is composed of three sub-factors: cognitive, motor, and non-planning impulsiveness. Higher scores indicate higher impulsivity. The internal consistency (Cronbach’s α) in this study was 0.65.
Korean Beck Anxiety Inventory (K-BAI)
The Beck Anxiety Inventory (BAI) developed by Beck et al. [20] was used, which was validated by Lee et al. [21]. This scale consists of 21 items rated on a 4-point Likert scale ranging from 0 to 3. Higher scores indicated higher levels of anxiety symptoms. The internal consistency (Cronbach’s α) in this study was 0.93.
Korean BDI-II (K-BDI-II)
The BDI-II developed by Beck et al. [22] and validated by Lim et al. [23] was used. It consists of 21 items rated on a 4-point Likert scale ranging from 0 to 3. The scale was composed of subscales measuring anxiety, concentration difficulties, and feelings of worthlessness. Higher scores indicated higher levels of depressive symptoms. The internal consistency (Cronbach’s α) in this study was 0.94.
State-Trait Anger Expression Inventory-Korean version
The Korean version of the State-Trait Anger Expression Inventory (STAXI-K) developed by Spielberger et al. [24] was validated by Chon et al. [25]. This scale consists of 44 items rated on a 4-point Likert scale, ranging from 1 to 4. It comprises five subscales: state anger experience (10 items), trait anger experience (10 items), anger-out (8 items), anger-in (8 items), and anger control (8 items). Higher scores indicate higher levels of each factor. The internal consistency (Cronbach’s α) in this study was 0.92, 0.96, 0.71, 0.88, and 0.82, respectively.
Procedure
Initially, permission was obtained from Holtzman et al. [16], the author of the BITe, to proceed with the Korean translation. The original scale was initially translated into Korean and then back-translated into English by a certified bilingual translator currently undergoing clinical training with a master’s degree in clinical psychology. This translated version was then reviewed by a team of five individuals, consisting of one clinical psychologist and four trainees holding a master’s degree in clinical psychology. The Korean version of the BITe can be found in Supplementary Table 1 (in the online-only Data Supplement).
Statistical analyses were performed using the following procedure: SPSS 25 (IBM Corp., Armonk, NY, USA) and AMOS 23 (IBM Corp., Armonk, NY, USA) were used to analyze the data. First, a frequency analysis and descriptive statistics were used to examine the demographic characteristics of the participants. Second, internal consistency (Cronbach’s α) and item-total correlations were examined to assess reliability. Third, Kaiser-Meyer-Olkin (KMO) and Bartlett’s tests were performed to validate whether the collected data were suitable for factor analysis. If the KMO value was above 0.5 and the Bartlett value was significant (p<0.05), the collected data were considered appropriate for the factor analysis [26]. Fourth, exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were conducted to confirm construct validity. In the EFA, maximum likelihood estimation was used for factor extraction, and direct oblimin rotation was performed. In CFA, the model fit of each factor structure model was examined using χ2, comparative fit index (CFI), Tucker-Lewis index (TLI), goodness-of-fit index (GFI), normed fit index (NFI), root mean square error approximation (RMSEA), and standardized root mean residual (SRMR). CFI, TLI, and GFI values greater than 0.90, NFI values greater than 0.95, RMSEA values less than 0.10, and SRMR values less than 0.08 were considered indicators of adequate fit [27-29]. Fifth, a correlation analysis was conducted to examine concurrent validity by examining correlations with variables such as anxiety, depression, anger, and impulsivity. Finally, Levene’s test, independent sample t-test, and one-way analysis of variance were conducted to confirm differences in BITe scores among sex, age, education level, and psychiatric disorder.
RESULTS
Demographic characteristics
Examining the demographic characteristics of the 296 participants, the average age of the total sample was 30 years (standard deviation [SD]=14.9). The sex distribution consisted of 73 female (24.7%) and 223 male (75.3%), indicating a higher proportion of male.
Upon examining BITe scores based on demographic characteristics, no significant differences were found between sex (F=0.20, p=0.65) and education (F=2.78, p=0.06). However, differences were observed among the age, with 10s exhibiting significantly lower BITe scores compared to individuals in their 20s and 30-40s (F=4.89, p<0.01). Furthermore, variations were identified based on the group of psychiatric disorder, with the stress related disorder group demonstrating significantly higher BITe scores than the psychotic disorder and other disorder groups (F=4.22, p<0.01). The other key descriptive statistics are presented in Table 1.
Reliability
Cronbach’s alpha was calculated to examine the internal consistency of the Korean version of the BITe. The internal consistency coefficient of the scale was 0.89, which was similar to the internal consistency of the original scale (0.88) [16]. Results of the item analysis are presented in Table 2. The item-total correlation coefficients (r) ranged from 0.73 to 0.84, and the Cronbach’s alpha values after item deletion ranged from 0.86 to 0.89.
EFA
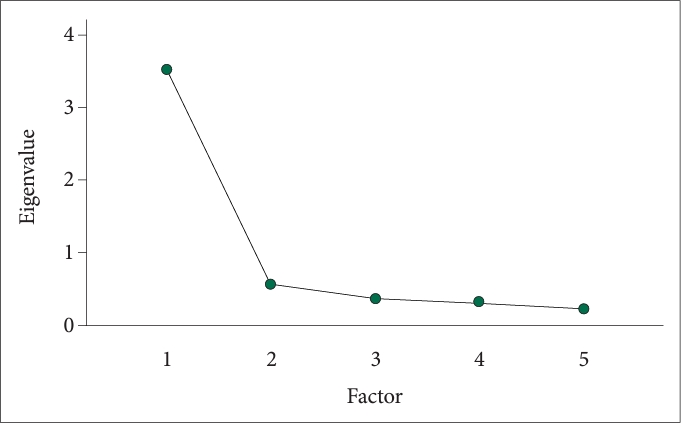
The KMO measure of sampling adequacy was 0.86, indicating a satisfactory sampling adequacy above the recommended threshold of 0.50. Bartlett’s test for sphericity was statistically significant (χ2=857.9, p<0.001), indicating an adequate level of correlation among the items for conducting EFA. Furthermore, using maximum likelihood estimation, factors with eigenvalues greater than 1 were extracted and analyzed using direct oblimin rotation. The analysis revealed that BITe accounted for 63.28% of the total variance in the single-factor dimension. Additionally, according to the scree plot (Figure 1), only the first factor had an eigenvalue greater than 1, whereas the eigenvalues decreased for subsequent factors (eigenvalue=3.52). These results suggest that a single-factor structure was appropriate for scale construction.
CFA
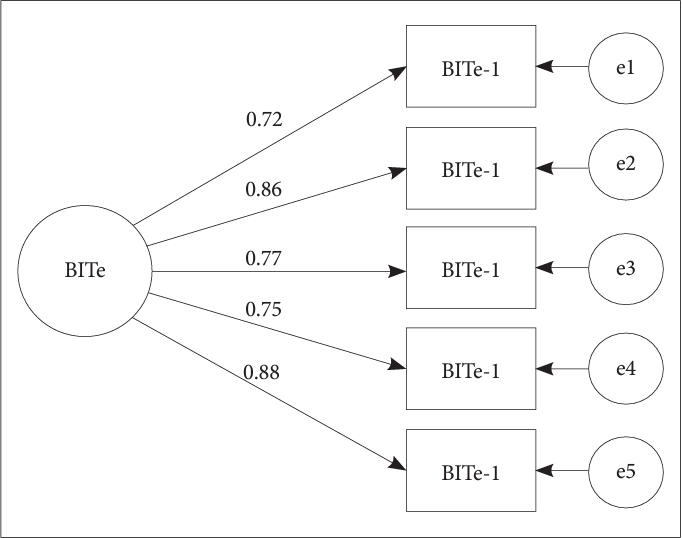
A CFA was performed to validate the single-factor model. The standardized regression coefficients resulting from the CFA are presented in Figure 2, and its fit indices are shown in Table 3. First, the fit indices, including CFI, TLI, NFI (>0.90), GFI (>0.95), and SRMR (<0.08), indicated an acceptable model fit [27,29]. In the original scale, only the GFI was reported, with a value of 0.99, similar to the present scale. However, the RMSEA value exceeded 0.1, possibly due to the model’s low degrees of freedom (df=5). RMSEA tended to show a poorer fit in models with lower degrees of freedom [30]. Overall, the model fit was considered acceptable.
Concurrent validity
Correlation analyses were conducted using relevant measures to assess scale validity (Table 4). First, the BITe showed significant positive correlations with depression (r=0.62, p<0.01), anxiety (r=0.41, p<0.01), trait anger (r=0.60, p<0.01), state anger (r=0.58, p<0.01), anger in (r=0.38, p<0.01), anger out (r=0.50, p<0.01), and impulsivity (r=0.42, p<0.01). However, there was a significant negative correlation with anger control (r=-0.21, p<0.01).
DISCUSSION
This study aimed to validate the Korean version of the BITe, originally developed by Holtzman et al. [16] in 2015, as a concise and accurate measurement of irritability. First, internal consistency was assessed to confirm the reliability. Cronbach’s α coefficient for this scale was 0.89, which is similar to Cronbach’s α coefficient of 0.88 calculated for the original scale. It is generally recommended that Cronbach’s α coefficient should be above 0.70, but some suggest that it should be above 0.80 when the scale has 3-10 items [31,32]. Considering that the Korean version of the BITe satisfies the more stringent cutoff proposed in previous studies, its internal consistency may be considered good. Furthermore, the item-total correlation coefficients in the item analysis ranged from 0.73 to 0.84, which was considered good when the coefficient was greater than 0.30 [33]. Therefore, the item-total correlations of the BITe may be considered acceptable. It is generally expected that as the number of items in a scale increases, the measurement error decreases and reliability increases [31]. Despite having a small number of items (five), the BITe demonstrated a reliable measurement of irritability. Therefore, it is expected that the BITe may stably assess irritability symptoms while reducing evaluation time and increasing efficiency.
Second, EFA and CFA were conducted to validate the construct validity of the Korean version of the BITe. Results of the EFA indicated that a unidimensional structure similar to that of the original scale was appropriate for constructing the scale. CFA demonstrated good fit indices, supporting the validity of the five-item unidimensional structure of the Korean version of the BITe. Given that the original study also supports a single factor, the validity of the single-factor scale is enhanced [16]. Irritability is widely used to describe a range of symptoms from non-pathological mood states associated with sleep deprivation to clear signs of psychiatric disorders. It has been measured using various scales without a clear conceptualization [6,7]. Therefore, the importance of accurately measuring irritability has been emphasized, and the BITe may be expected to accurately measure irritability symptoms in a single dimension.
Third, concurrent validity was examined by investigating correlations between the BITe and measures of depression, anxiety, anger experience and expression, and impulsivity. The BITe showed significant positive correlations with depression, anxiety, trait anger, state anger, anger in, anger out, and impulsivity. Furthermore, a significant negative correlation was observed with anger control. These findings are consistent with previous research suggesting that irritability is associated with emotional distress, such as depression and anxiety, and is frequently observed as a symptom in patients with depression and anxiety disorders [9-11]. Additionally, irritability is defined as experiencing negative emotions such as anger, occasionally leading to verbal or behavioral anger outbursts and difficulties in impulse control, which is consistent with previous research showing that irritability is frequently observed in disorders where individuals display language or behavioral anger outbursts and have difficulties in impulse control [5,12-14]. Irritability is frequently characterized as a behavioral expression of anger. Moreover, given prior research showing a correlation between irritability, impulsiveness problems, and externalization disorders, the negative correlation with anger control aligns with expectations [1-4,34]. These findings confirm that irritability may be one of the core symptoms of various mental disorders included in the DSM-5 [7]. Considering the universality of irritability as a symptom across different mental disorder categories, the BITe might be useful in assessing irritability in patients with psychiatric disorders in clinical settings, facilitating the evaluation of symptom severity and monitoring of progress. Moreover, using the BITe to specifically investigate the mechanisms underlying the relationship between irritability and commonly associated psychiatric symptoms such as depression, anxiety, anger, and impulsivity may be helpful in developing more effective treatment plans for patients with irritability symptoms. A common therapeutic intervention is cognitive-behavioral therapy, targeting hostile attribution biases and cognitive processes [35,36]. Recently, interpretive bias program has focused on cognitive retraining to link ambiguous facial expressions to positive emotions [36,37].
Finally, while examining BITe scores across demographic characteristics (sex, age, education level, and disorder group), no significant differences were observed based on sex and education level. However, there was a difference in age emerged, with teenagers exhibiting significantly lower BITe scores compared to other age groups. This contrasts with irritability typically prompting mental health visits in children and adolescents. This outcome might be influenced by recruiting participants starting from age 18, approaching early adulthood. Additionally, BITe scores varied across psychiatric disorder groups, with the stress-related disorder group showing significantly higher scores than the psychotic disorder and other disorder groups. This underscores the close association between stress and irritability, as stress-induced cortisol secretion can impact the emotion-regulating brain area, potentially leading to irritability [38]. In a previous study, irritability emerged as a key symptom in the post-traumatic stress disorder patient group and was identified an important indicator of clinical severity and risk of suicide [39]. Considering these findings, an emotion-regulating intervention focused on irritability may be considered for individuals experiencing recent stress events.
The limitations of this study and suggestions for future research are as follows: first, since the study was conducted on outpatients and inpatients with psychiatric disorders, there are limitations to generalizing its results to a representative sample of the general population. Second, a limitation arises from a skewed sex distribution with 75.3% male. However, since there is no significant difference in irritability based on sex, generalizing the findings to all sex is deemed reasonable. Third, this was a cross-sectional retrospective study and did not include a follow-up period or evaluate the test-retest reliability. Therefore, sampling with consideration for the general adult population and longitudinal studies may be necessary. Despite these limitations, this study is significant in validating the Korean version of the BITe and confirming that it is a psychometric measurement tool that can quickly and accurately assess irritability in clinical populations.