INTRODUCTION
Cancer is a leading cause of death worldwide, and the rapid increase in its number of cases can be primarily attributed to the promotion of lifestyle behaviors that increase cancer risk [1]. Along with the multiple physical complications it causes, cancer is also the source of major psychosocial problems [2]. Similar to other chronic diseases, it is a common cause of fear in patients, owing to fear of the illness [3,4] or disease progression [5].
Fear of progression is one of the most common afflicting symptoms experienced by cancer patients [6]. It is an expected reaction that can become dysfunctional or problematic if present in high levels [7,8], which can negatively impact the patientŌĆÖs quality of life [9,10]. This manifests as patients become alert at the appearance of the slightest symptoms and try to gather all the relevant information about them, subsequently insisting on unnecessary laboratory workups [11].
However, cancer not only affects the flow of a patientŌĆÖs daily life, but also causes sleep disturbances that may enhance their fear of progression [12], which creates dysfunctional sleep beliefs in cancer patients. When experiencing sleep disturbance [13], they tend to think ŌĆ£My immune system will have serious problems if I donŌĆÖt go to sleep at a certain timeŌĆØ or ŌĆ£If I donŌĆÖt sleep well at night, my cancer may recur or metastasize.ŌĆØ Sleep disturbances are associated with psychological distress, causing patients to worry about its effect on their immune systems [14], which are reportedly damaged from sleep deprivation, thereby indirectly promoting cancer progression [15]. Subsequently, patients become tormented about the impact that sleep disturbances might have on cancer progression [14]. Therefore, cancer-related sleep beliefs are dysfunctional, as they increase the apprehension of cancer patients and consequently aggravate sleep problems [16].
Apart from dysfunctional sleep beliefs, dysfunctional self-focus may also become problematic, which refers to a phenomenon or state in which attention is turned toward oneself. This behavior can either be functional or dysfunctional, which influences the psychology of the person through several aspects like self-rumination and self-reflection [17]. Examples of dysfunctional self-focus are ŌĆ£Negative thoughts only arise when you focus inwardŌĆØ or ŌĆ£Looking into my feelings or actions makes them more unpleasant.ŌĆØ In contrast to rumination, which is a response style in which someone continues to recall negative emotions or unresolved past problems, dysfunctional self-focus starts from a cognitive process of self-consciousness, which is necessary for inner perceptions and reflections [18]. Previous research show that dysfunctional self-focus worsens the psychological stress that is associated with stressful situations [19]. Therefore, dysfunctional self-focus may contribute to depression, which can lead to self-focus becoming maladaptive [20].
Dysfunctional self-focus is the result of several medical or psychological problems, but literature regarding this topic is scarce. Further research is necessary to obtain a better understanding of the potential triggers for this dysfunction and its impact on a patientŌĆÖs life. No previous studies have focused on dysfunctional self-focus among cancer patients. Nevertheless, there are indications that cancer patients tend to have excessive self-focus [21], which may result in increased worry about their disease state and progress. As cancer significantly affects several human abilities, research on its impact on dysfunctional self-focus is necessary to gain clearer insights into the mechanism through which this dysfunction occurs.
We explored whether cancer patientsŌĆÖ dysfunctional self-focus is a significant contributor to their fear of progression. In addition, their psychiatric symptoms such as depression, anxiety, insomnia, and cancer-related dysfunctional sleep beliefs may mediate the relationship between these factors. We posited that 1) cancer patientsŌĆÖ dysfunctional self-focus would be positively associated with their fear of progression, 2) dysfunctional beliefs about sleep would be positively associated with fear of progression, 3) psychiatric symptoms would be positively correlated with fear of progression, and 4) psychiatric symptoms might mediate the relationship between dysfunctional self-focus and sleep beliefs and fear of progression.
METHODS
Participants and procedure
We conducted a retrospective review of cancer patientsŌĆÖ medical records who were visiting the Stress Management Clinic for cancer patients in the Asan Medical Center for the first time in Seoul, South Korea from March to September in 2022. Cancer patients aged from 18-79 years old were included. Patients who 1) were unable to move by themselves, 2) had serious medical or organic disease that impaired cognitive functioning, 3) had delirium or major psychosis, 4) were unable to complete the self-rating scales, or 5) had a problem in communication were excluded. All 196 cancer patientsŌĆÖ medical records were reviewed and information on age, sex, types of cancer, cancer stage, current treatment modalities, history of surgical procedures, and responses to rating scales was collected. The studyŌĆÖs protocol was approved by the Asan Medical Center Institutional Review Board (2023-1019).
Measures
Fear of Progression Questionnaire-Short Form
The Fear of Progression Questionnaire (FoP-Q) is a self-rating scale used to measure oneŌĆÖs fear of progression [22] of chronic illness. The original version included 43 items, and a 12-item shortened version [23]. A higher total score reflects a higher level of fear of disease progression. We applied the Korean version of the FoP-Q-Short Form (FoP-Q-SF) [24].
Dysfunctional Self-focus Attribution Scale
The Dysfunctional Self-focus Attribution Scale (DSAS) is a self-rating scale that can assess oneŌĆÖs level of dysfunctional self-focus [18]. It includes 15 items which can be scored on a 5-point Likert-type scale and are clustered into three parts: 1) negatively biased focus (items 2, 5, 7, 12, and 15), 2) low clarity awareness (reverse scoring: items 1, 3, 6, 8, and 9), and 3) low focus control (items 4, 10, 11, 13, and 14). A higher total score reflects a higher degree of dysfunctional self-focus. We applied the original Korean version.
Patient Health Questionnaire-9 items
The Patient Health Questionnaire-9 items (PHQ-9) is a self-rating scale that can be used to measure the severity of depression [25]. It contains 9 items, which range from 0 (not at all) to 3 (nearly every day). A higher total score reflects a severe level of depression. We applied the Korean version of the PHQ-9 [26].
State subcategory of the State and Trait of Anxiety Inventory
The State subcategory of the State and Trait of Anxiety Inventory (STAI-S) is a part of a STAI, a self-rating scale that can be used to measure oneŌĆÖs anxiety [27]. The STAI can measure the state and trait level of oneŌĆÖs anxiety, and we applied the state subcategory of the STAI. It contains 20 items, which range from 1 (not at all) to 4 (very much so), and a higher total score reflects a higher level of state anxiety. We applied the Korean version [28].
Cancer-related Dysfunctional Beliefs about Sleep scale
The Cancer-related Dysfunctional Beliefs about Sleep scale (C-DBS) is a self-rating scale that can be used to measure oneŌĆÖs level of cancer-related dysfunctional beliefs about sleep [13]. It consists of 2 items, which can be rated on a 0-10 scale, and a higher total score reflects a higher level of dysfunctional beliefs about sleep. We applied the original version developed in Korean.
Statistical analysis
Demographic characteristics with a continuous value and rating scale scores were summarized as means┬▒standard deviations, and categorical variables were summarized as number (%). We defined clinical significance as a two-tailed significance level of 0.05. PearsonŌĆÖs correlation coefficients were calculated to examine whether cancer patientsŌĆÖ fear of progression is significantly correlated with demographic variables and rating scale scores included age, DSAS, PHQ-9, STAI-S, ISI, C-DBS, and NRSs of pain and fatigue. Linear regression with enter methods was done to explore which variables can predict the FoP-Q-SF score. To examine whether the influence of dysfunctional self-focus on fear of progression could be mediated by psychological distress, the bootstrap method was implemented with 2,000 resamples. Statistical analysis was done using SPSS version 21.0, AMOS version 27 for Windows (IBM Corp., Armonk, NY, USA), and Jamovi version 1.6.18.0 (https://www.jamovi.org).
RESULTS
We collected the information of 196 cancer patients. Among them, the mean age was 57.5┬▒14.0 years old, 67.9% were female, and 83.2% were married (Table 1). In terms of cancer types, 92.9% were solid tumors and 7.1% were hematologic malignancy. Among patients with cancer types with TNM classification (n=179), 34.1% had been diagnosed as stage IV. Among the patients, 45.9% had been diagnosed as having major depressive disorder or adjustment disorder, 30.6% as having insomnia disorder, and 15.8% as having anxiety disorders or somatic symptoms disorders.
Table 2 shows the PearsonŌĆÖs correlation coefficients among the symptom rating scales. Young age was significantly correlated with high FoP-Q-SF (r=-0.17, p=0.021) scores. High FoP-Q-SF scores were significantly correlated with high PHQ-9 (r=0.60, p<0.001), STAI-S (r=0.38, p<0.001), ISI (r=0. 34, p<0.001), C-DBS (r=0.47, p<0.001), pain-NRS (r=0.24, p<0.001), fatigue-NRS (r=0.37, p<0.001), and DSAS (r=0.58, p<0.001) scores.
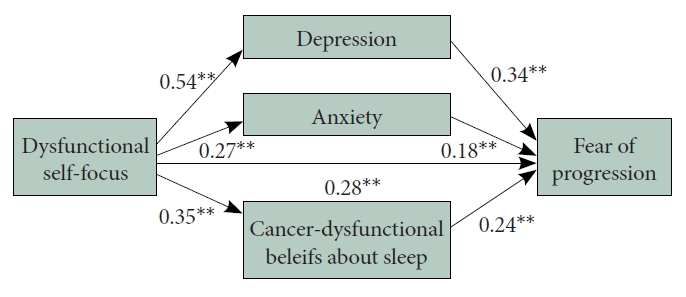
Linear regression analysis with enter methods was done to explore predictive variables for fear of progression. The FoP-Q-SF score was predicted by young age (╬▓=-0.13, p=0.011), PHQ-9 (╬▓=0.36, p<0.001), STAI-S (╬▓=0.18, p=0.001), C-DBS (╬▓=0.22, p<0.001), and DSAS (╬▓=0.25, p<0.001) (Table 3). Mediation analysis showed that dysfunctional self-focus directly influenced patientsŌĆÖ fear of progression. In addition, cancer patientsŌĆÖ depression, anxiety, and cancer-related dysfunctional beliefs about sleep mediated this relationship (Table 4 and Figure 1).
DISCUSSION
We observed that young age, depression, state anxiety, cancer-related dysfunctional beliefs about sleep, and dysfunctional self-focus were significant variables affecting fear of progression. Furthermore, dysfunctional self-focus directly influenced cancer patientsŌĆÖ fear of progression, and their depression, anxiety, and cancer-related dysfunctional sleep beliefs mediated the relationship between dysfunctional self-focus and fear of progression.
Fear of progression was relatively high with a mean score of 35.5┬▒12.1. Results were similar to those of studies of lung cancer patients, known to be a cancer with relatively high levels of fear of progression [31]. It has been reported that cancer patients who are relatively young, single, and have undergone chemotherapy tend to have a higher fear of cancer progression [32]. Furthermore, a meta-analysis found a weak but significant relationship between fear of cancer recurrence and chemotherapy treatment in cancer patients [33]. Less than half of the participants in this study were receiving chemotherapy, which may account for the high level of fear of progression. Many patients diagnosed with cancer experience uncertainty and fear about the future. In particular, young cancer patients have a high fear of cancer recurrence due to low survival rates and a high risk of secondary cancers [34]. In a study of 247 adolescents and young adults, the majority reported high levels of fear of progression. Consistent with previous research [31,32], young age was identified as a predictor of fear of cancer progression. Therefore, age should be considered when developing fear of progression interventions.
Anxiety and depression in cancer patients were correlated and predictors of fear of progression. Cancer patients with a high level of fear of progression are more anxious and depressed. These findings are consistent with those of previous research [33,35]. Depression may influence cancer patientsŌĆÖ fear of progression in various ways [36] and may weaken the patientŌĆÖs coping strategies [37]. Anxiety runs parallel with fear of progression [38], since both emotions are natural and adaptive responses to perceived threats or danger. Despite the fact that fear of progression appears to be a distinct phenomenon in the clinical setting, it shares some characteristics with anxiety disorders when it comes to psychological and somatic burdens [39]. Furthermore, catastrophizing thinking [40] or intolerance of uncertainty [41] related to viral anxiety influenced fear of progression among cancer patients during the coronavirus disease-2019 (COVID-19) pandemic. Thus, patients with high level of fear of progression may require more active psychological support, as anxiety and depression may afflict them.
Consistent with previous research on lung resection patients [31], cancer-related dysfunctional beliefs about sleep were correlated with and predictive of fear of progression in this study. Previously, we reported that cancer-related dysfunctional beliefs about sleep mediated the influence of sleep disturbance on fear of progression among lung cancer patients [31]. In addition, cancer-related dysfunctional sleep beliefs mediated the influence of viral anxiety on cancer patientsŌĆÖ fear of progression during the COVID-19 pandemic [14]. We found that cancer patients may be affected by dysfunctional beliefs about sleep and fear of progression can have a serious impact on a cancer patientŌĆÖs quality of life [42]. Therefore, patients with high levels of fear of progression should be screened and interventions should be implemented.
It should be noted that the level of dysfunctional self-focus in cancer patients in this study was elevated, as indicated by an average mean of 44.9 with a standard deviation of 8.7. Such high rates can also be seen in relation to various psychiatric problems in cancer patients, with the highest mean pertaining to major depressive disorder or adjustment disorder (90 [45.9%]), followed by insomnia disorder (60 [30.6%]), anxiety disorder or somatic symptoms disorder (31 [15.8%]), and others (15 [7.7%]). Unfortunately, the research about the relationship between dysfunctional self-focus and cancer is sparse, which prevents us from supporting these high rates with significant past findings. Limited existing research on the association between dysfunctional self-focus and cancer thus hinders our ability to substantiate these elevated rates with prior significant evidence.
The Pearson correlation between dysfunctional self-focus and each of the psychological problems (depression, anxiety, insomnia) and fear of progression was positive, indicating the association between dysfunctional self-focus and psychological problems in cancer patients. As was mentioned, lack of research on this subsequently prevents comparison with other results. Moreover, even after accounting for all other variables in the linear regression analysis, the relationship between dysfunctional self-focus and fear of progression persisted. Furthermore, as per the mediation analysis, it appears that dysfunctional self-focus exerts a direct impact on fear of progression in cancer patients. These interrelated factors can potentially establish a harmful cycle, wherein cancer patients may experience dysfunctional self-focus, psychological problems, and fear of progression, perpetuating their distress. Presently, no investigation on the connection between dysfunctional self-focus, psychological issues, and fear of progression among cancer patients have been made. However, based on the studyŌĆÖs findings, it is evident that the fear of progression experienced by cancer patients may be impacted by their psychological problems. Recognizing that psychological problems can be modified, addressing these issues could potentially enhance quality of life for individuals with cancer.
There are limitations to this study. First, a small sample of 196 cancer patients from a single medical center may restrict the generalizability of the findings to the broader population of cancer patients. Second, we utilized a retrospective medical records review, which may have introduced recall bias and limited the ability to establish causality. Third, we collected participantsŌĆÖ information from a clinically heterogeneous sample regarding cancer types and stages. The subjects were patients at the Stress Management Clinic at a tertiary hospital, and most had been diagnosed as having psychiatric disorders or sleep disorders. We must consider the possibility of selection bias in that it is possible that the level of psychological distress of the participants in this study may have been higher than that of cancer patients who had not visited the clinic. Last, we measured psychological distress using self-reported rating scales, not using structured interview tools. However, we collected clinical information thoroughly and investigated whether the patients had had their psychiatric disorders diagnosed by two qualified psycho-oncologists to overcome these limitations.
In conclusion, we observed that dysfunctional self-focus may influence cancer patientsŌĆÖ fear of progression with the mediation of depression, anxiety, and cancer-related dysfunctional beliefs about sleep. The findings highlight the importance of assessing and addressing dysfunctional self-focus alongside signs of psychological distress, such as fear of progression, depression, anxiety, and dysfunctional beliefs about sleep, in cancer patients. Healthcare providers should consider incorporating routine psychological screening and interventions into cancer care to improve patientsŌĆÖ overall well-being.