INTRODUCTION
White matter lesions (WMLs) are commonly found in the T2-weighted magnetic resonance imaging (MRI) or fluid-at-tenuated inversion recovery (FLAIR) scans of normal elderly people.1 WMLs also have been found in Alzheimer's disease (AD),2 vascular dementia,34 and depression,567 and have been associated with vascular risk factors such as hypertension and diabetes.89 Neuropathologically, WMLs are characterized by the demyelination of white matter axons, mild fibrillary gliosis, and fibrohyaline thickening of small vessels that supply the white matter.1011 In particular, irregular periventricular WMLs and deep WMLs have been associated with microcystic infarcts and patchy rarefaction of the myelin, which are ischemic in nature.1213 These findings support a prominent role of vascular factors in the pathogenesis of WMLs.
Pathological evidence suggests that WMLs may play a role in the clinical symptoms of AD. Individuals with more WMLs have a higher risk of developing AD.1415 In addition, WMLs are associated with cognitive dysfunction and the severity of the dementia.1617 However, the relationship between depression and WMLs in AD remains unclear. Several studies have explored the relationship between WMLs and depression. WMLs, particularly in the frontal area, have been found to be associated with higher depression scores.1820 Other studies, however, did not find such a relationship.212223 The heterogeneity of the study populations, the methods by which depression was assessed, and the measurements of the WML volumes might contribute to these inconsistent results. In most studies, different semi-quantitative visual rating scales, such as Fazeka's scale and Scheltons's scale, were used.1819212223 In one study, an automated volumetric method was used to assess WML volumes, but depression was assessed by rating scales rather than by clinical diagnosis.20 In other studies, depression was assessed by clinical diagnosis, but WMLs were assessed by visual rating scales.2122
The present study avoided some of the limitations of these previous studies by 1) using automated quantitative volumetric methods to assess the severity and location of WMLs; 2) using both a structured clinical interview and a self-report questionnaire to diagnose the presence and severity of depression; and 3) recruiting only AD patients to avoid a confounding effect from a heterogeneous study population.
The purpose of this study was to explore the relationship between depression and the severity and location of WMLs in patients with AD. We tested the hypothesis that larger WML volumes and frontal WMLs in particular are associated with depressive mood and clinician-diagnosed depression in patients with AD.
METHODS
Subjects
We recruited AD patients from a dementia clinic (Seoul National University Bundang Hospital, SNUBH) and communities [the Korean Longitudinal Study on Health and Aging (KLoSHA)24 and the nationwide dementia screening and registry program (DSRP)]. All subjects underwent standardized clinical interviews and neurological and physical examinations, which were administered by four geriatric psychiatrists with advanced training in neuropsychiatry and dementia research according to the protocol of the Korean version of the Consortium to Establish a Registry for Alzheimer's Disease clinical assessment battery (CERAD-K),25 the standardized TIA/stroke form from the Atherosclerosis Risk in Communities Study (ARIC),26 and the Mini International Neuropsychiatric Interview (MINI),27 to diagnose dementia, stroke, and major psychiatric disorders, respectively.
Dementia was diagnosed in these participants in accordance with the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria,28 and probable or possible AD was diagnosed according to the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association (NINCDS-ADRDA) criteria.29 A total of 93 subjects met the inclusion criteria. Sixty-six (71%) subjects had probable AD and 27 (29%) had possible AD.
All the participants were fully informed regarding their study participation and either the participant or a legal guardian provided written informed consent. The study protocol was approved by the Institutional Review Board of SNUBH.
Assessment of depression
Depression was evaluated based on information provided from the patients as well as information provided by their primary caregiver. First, we administered a self-report questionnaire, the Korean version of the Geriatric Depression Scale (GDS-K), to assess subjective depressive mood.30 Second, research-trained psychiatrists interviewed the patients and(or) primary caregivers using the MINI to clinically diagnose depression.27 The severity of depression was rated from very mild (subsyndromal depression) to moderate-to-severe depression (e.g., minor and major depressive disorder, dysthymic disorder).
Major depressive disorder (MDD) and dysthymic disorder were diagnosed according to the DSM-IV criteria, and minor depressive disorder (MnDD) was diagnosed according to the research criteria proposed in the DSM-IV. Subsyndromal depression (SSD) was diagnosed according to the following operational criteria: 1) two or more symptoms listed in the DSM-IV criterion A for a major depressive episode occurring during the same two-week period; 2) at least one symptom should be depressed mood or anhedonia; 3) each depressive symptom should be present for more than half of one day or more than seven days during the 2 weeks; and 4) symptoms do not meet the criteria for a diagnosis of MDD or MnDD. Subjects were divided into two diagnostic group: 1) Depression, which was defined as evidence of MDD, MnDD, dysthymic disorder, or SSD or 2) No depression, which was defined as no current evidence of significant depressed mood.
Assessment of neuropsychological functions
Global cognitive function was evaluated using the Mini-Mental Status Examination (MMSE).2531 To assess memory function, the word list memory test (WLMT), the word list recall test (WLRT), and the word list recognition test (WLRcT) from the Korean version of the CERAD Neuropsychological Assessment Battery (CERAD-K-N) were administered. Language function was evaluated using the verbal fluency test (VFT) and the 15-item modified Boston Naming Test (mBNT) from the CERAD-K-N.2531 Visuospatial function was evaluated using the constructional praxis test (CPT) from the CERAD-K-N.2531 Frontal function was evaluated using the trail making test-A/B (TMT-A/B) from the CERAD-K-N.2531 All the assessments were performed at SNUBH
Assessment of WMLs
T1-weighted MR and FLAIR images were acquired on a 3.0 Tesla MRI scanner system (Achieva, Philips Medical System, The Netherlands) at SNUBH. The T1 images were acquired using the following protocol: magnetic field=3.0 Tesla; sequence=SPGR; repetition time/echo time=22/4 msec; number of excitations=1; flip angle=40°; field of view=240 mm; plane=sagittal; matrix=256×256 mm; thickness=1 mm; inter-slice gap=none; slice number=120. The FLAIR images were acquired using the following protocol: magnetic field=3.0 Tesla; repetition time/echo time=9900/160 msec; number of excitations=1; flip angle=90°; field of view=240 mm; axial plane matrix=256×256 mm; thickness=3 mm; and inter-slice gap=none.
All the processes were implemented in Matlab 2010a (The MathWorks, Inc., Natick, MA, USA). WMLs were automatically segmented from the FLAIR images according to the method adopted by Yoo et al.32 A study-specific T1 template (SST) was constructed for accurate spatial normalization using the DARTEL toolbox in SPM8 (Wellcome Trust Centre for Neuroimaging, London, UK; http://www.fil.ion.ucl.ac.uk/spm). All the T1 images, as well as the FLAIR and segmented WML images, were spatially transformed to the SST.
To define the regions to be classified as WMLs, a mask-labeled region was manually delineated from the MNI standard space by one neurological expert. Frontal, temporal, parietal, and occipital WML regions were defined. The MNI152 standard T1 image as well as the mask-labeled region was spatially transformed to the SST. Sub-classified WML images were obtained by applying the transformed mask to the segmented WML images through voxel-wise image multiplication for each individual WMH image. The sub-classified WMH volumes then were computed by counting the voxels from the labeled WML images.
Statistical analysis
We computed descriptive statistics on the demographic variables and disease-related measures using independent t-tests for each continuous variable and chi-square tests for each categorical variable to examine the differences between the groups. The neuropsychological measures between the groups were compared by an analysis of variance with adjustments for age, education, and GDS-K scores, which are well-established risk factors for cognitive dysfunction.313334 We used a logarithmic transformation to produce normally distributed WML volumes. The associations between the log-transformed WML volumes and clinical variables were examined using Pearson's correlation coefficient or Spearman's rank-order correlation coefficient (r) as appropriate. We also performed multivariate logistic regression analyses. First, we conducted unadjusted analyses examining the relationship between log WML volumes and the dependent variables. Second, we included two sets of adjustment variables: 1) those characteristics well-known to influence depression, i.e., age, gender, and level of education3536 and 2) vascular risk factors (e.g., cardiovascular disease, hypertension, diabetes)37 and prior depression history.3839 Due to the high correlation between the total WML volume and regional WML volumes, separate models were generated to analyze the relationship between depression and WML volume by location. For all the analyses, a two-tailed p-value of less than 0.05 was considered statistically significant. All the analyses were conducted using SPSS version 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
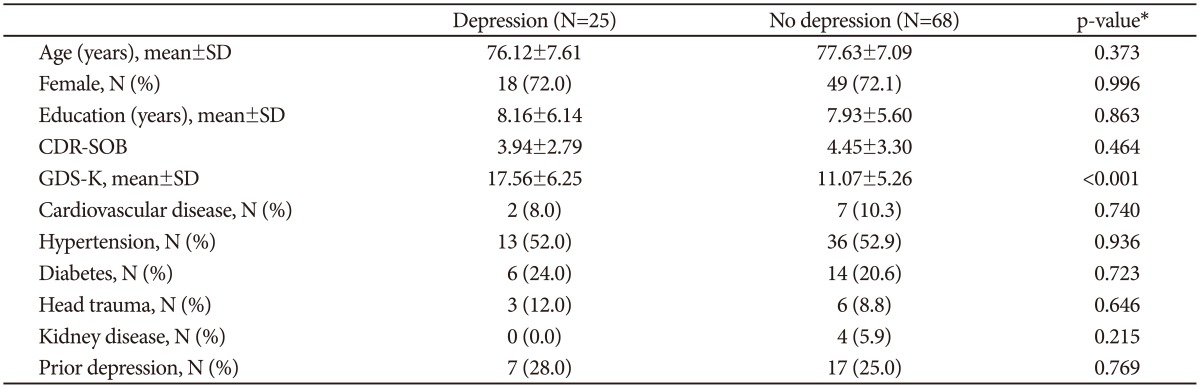
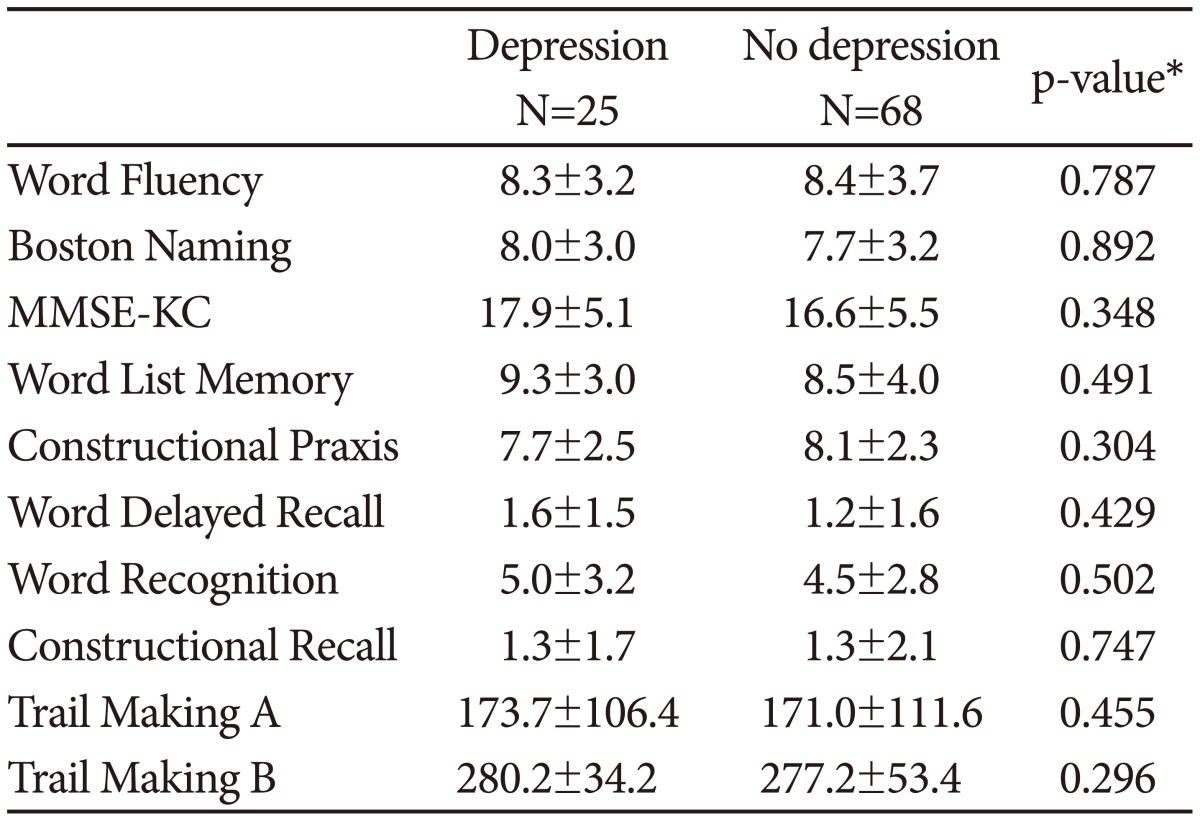
The clinical and demographic characteristics of the participants are summarized in Table 1. Of the 93 subjects, 25 were diagnosed with depression and 68 were assigned to the no depression group. No differences between the groups were observed on any clinical or demographic variables except GDS-K scores. The neuropsychological performance of the participants is summarized in Table 2. No differences were observed between the depression and no depression groups.
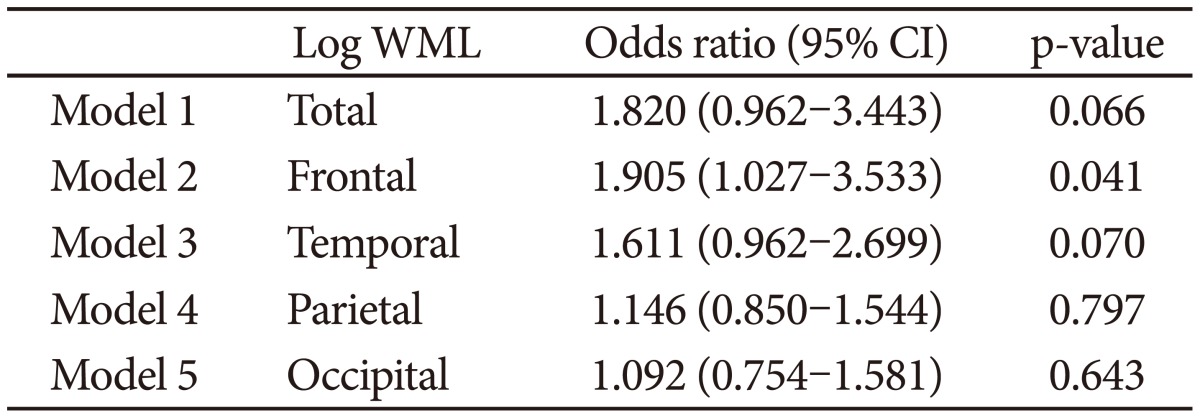
We performed multiple logistic regressions to assess the relationship between clinician-diagnosed depression and the total and regional WML volumes with adjustments for potential confounding effects of vascular risk factors and residual clinical variables. The total log WML volume was not significantly associated with the presence of clinician-diagnosed depression (odds ratio 1.820, 95% CI 0.962-3.443, p=0.066). When the WML volumes were analyzed separately with respect to location, the log frontal WML volume was significantly associated with the presence of clinician-diagnosed depression (odds ratio 1.905, 95% CI=1.027-3.533, p=0.041), but no significant relationship was observed in any other WML region (Table 3).
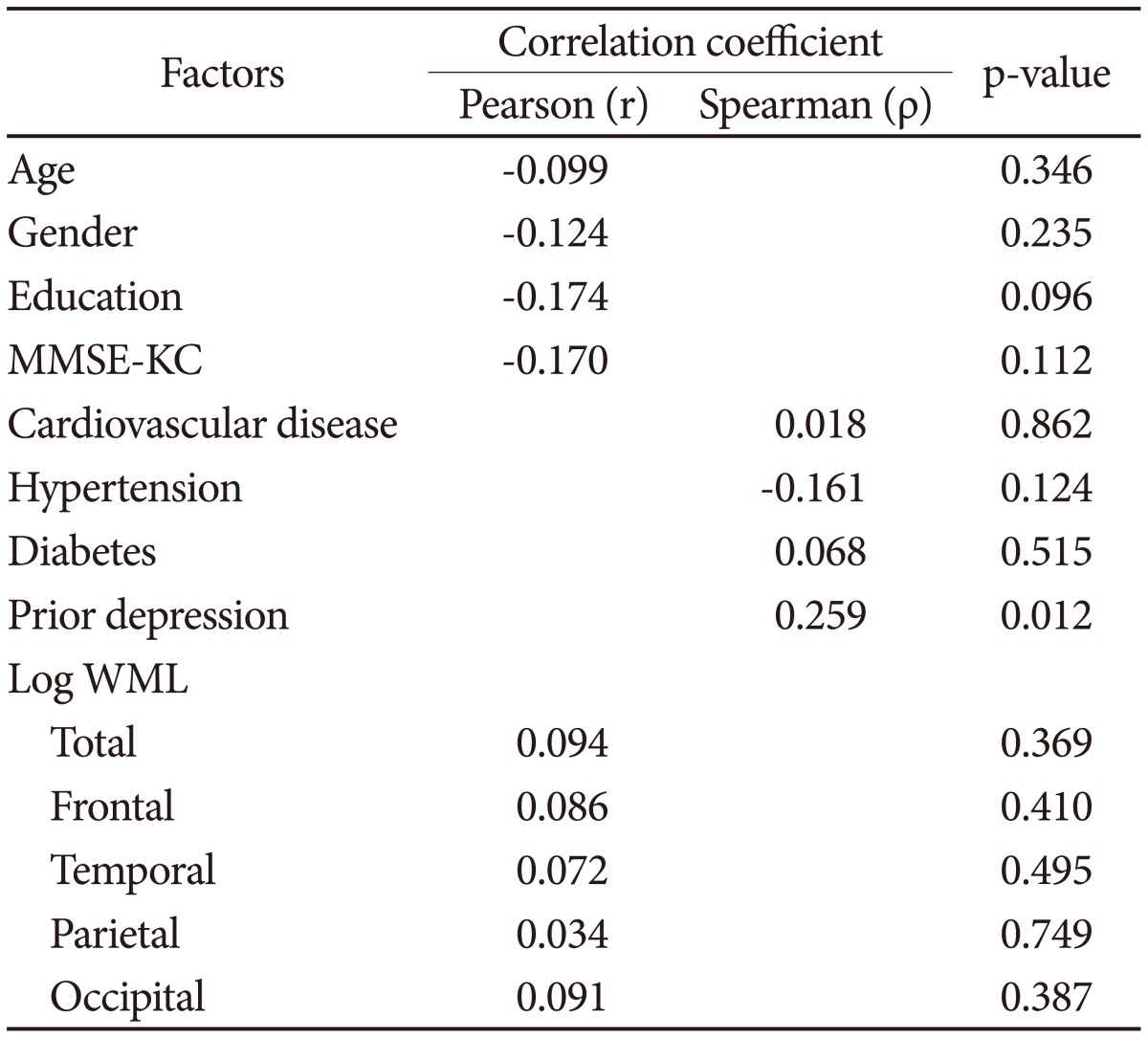
Table 4 shows the relationship between the GDS-K scores as well as other clinical variables and the log total or regional WML volumes. The GDS-K scores were not associated with either the log total WML volume (p=0.369, Pearson's chi-squared test) or the log frontal WML volume (p=0.410, Pearson's chi-squared test).
DISCUSSION
Depression has been recognized as one of the most frequent psychiatric comorbidities of AD, and previous studies have suggested that 20% to 50% of patients with AD suffer from depression.404142 The importance of depression in AD is underscored by its negative impact on the patient's quality of life,43 cognitive ability,44 and activities of daily living45 as well as the caregiver's stress and psychological comorbidity.46 Short-term mortality in elderly subjects with less severe dementia is predicted by the presence of subsyndromal depression and mood symptoms.47 Identifying and treating patients with depression in AD may reverse this associated morbidity.
The etiologies and pathophysiology of depression in AD remains unclear. Depression can be organic in nature due to cerebrovascular changes.548 The neurodegenerative process may directly contribute to the development of depression. Several studies have found that depression has been associated with the loss of noradrenergic or serotonergic nuclei4950 or as a consequence of low-grade inflammation in the brain.51
In our study, the WML volume, especially the frontal WML volume, was positively and independently correlated with depression after adjusting for vascular risk factors. This result is consistent with some previous studies.181920 The WMLs are a surrogate marker of small-vessel vascular disease resulting from ischemic damage due to chronic hypoperfusion, whereas mild periventricular WMLs are non-ischemic in origin. Recently, Brickman et al.52 reported that reduced cerebral autoregulation was associated with an increased WML volume. There is growing evidence that frontal and subcortical WMLs are implicated in late-life depression and influence the outcome, possibly via the disruption of frontal-subcortical circuits.25354 These findings, together with those in the present study, suggest that vascular depression can be considered an etiology of depression in AD. WMLs may affect mood symptoms via the disruption of intracerebral connectivity, compromising efficient neuronal communication. The prefrontal cortex and its extensive cortical-cortical and cortical-subcortical connectivity is thought to play a central role in motivation-based depressive symptoms in dementia.55
The results from previous studies have been inconsistent with respect to the relationship between WMLs and depression in AD. Several factors may contribute to these inconsistencies.
First, different visual rating scales were used across studies,1819212223 and therefore scores from different rating scales are not directly comparable. Different visual rating scales can produce inconsistent results among neuroimaging studies.56 Furthermore, visual rating scales are less sensitive than volumetric methods.57 Soennesyn et al.20 used both automated volumetric WML measurement and a visual rating scale, and reported that the automated volumetric measure of the total and frontal WMLs but not the visual rating scale scores were associated with the severity of depressive symptoms. This finding suggests that visual rating scales inevitably have some limitations such as data nonlinearity, lack of sensitivity to small changes, and susceptibility to ceiling effects.85859
Second, the methods to assess depression were different across studies. Diagnosing depression in AD remains problematic for several reasons. First, the symptoms of depression in AD overlap with other neuropsychiatric manifestations of dementia. The use of rating scales in a patient with dementia without consideration of this overlap in nonspecific depressive symptoms may result in an erroneous assignment of a depression diagnosis in AD.60 Second, another complicating factor in the diagnosis of depression in AD is the patient's limited ability to communicate distress coherently. Patients with dementia cannot always accurately report their own symptoms, and therefore may underreport their symptoms.61 AD patients may also perceive themselves as less depressed than do their caregivers or a clinician.62 Third, depressive symptoms in patients with AD differ from those in depressed but otherwise cognitively normal elderly patients. Patients with AD appear to have more motivational symptoms and delusions and less commonly experience sadness, sleep disturbance, and appetite loss.416364 Fourth, there are currently no standardized methods to diagnose depression in AD. The recommendation for diagnosing depression in AD is to use a structured psychiatric interview; depression scales should be used to rate the severity of the depression but not to diagnose. In our study, we used both a self-rating depression questionnaire and a structured psychiatric interview to assess depression. Interestingly, we found a significant association between clinician-diagnosed depression and WML volumes but failed to show such a relationship between self-reported depression scores and WML volumes.
The heterogeneity of the study populations may also contribute to the inconsistent results across studies. Some studies included only patients with AD,2122 but other studies included patients with other types of dementia such as vascular dementia, dementia with Lewy bodies, and frontotemporal dementia as well as AD.18192023
The prevention or reduction of WMHs could lessen the burden of depression and depressive symptoms in patients with dementia. The presence of WMLs, in particular in the frontal area, is associated with depression in AD, which implies a common pathophysiology of depression caused by disruption to the frontal-subcortical circuits. Understanding the pathogenesis is important and may offer important insights into therapeutic options for the treatment and prevention of depression in AD.
To our knowledge, this is the first study to investigate the association between depression and WMLs in AD using a standardized structured psychiatric interview to assess depression and an automated quantitative measurement to assess the severity and location of WMLs. However, this study was cross-sectional in design and the depression group was relatively small, which may warrant a prospective study on a larger sample to confirm the positive correlation between WMLs in AD and depression and investigate its clinical significance.