Sir,
Noh et al.1 reported the finding that a significant association between current smoking and depression was only observed in females by adjusting several confounders. The authors dealt with enough number of subjects, aged from 45 to 105 years old, and depression was judged by 10-item scale of Center for Epidemiological Studies-Depression (CES-D 10). Although they also measured alcohol use to know the association with depression, I want to make an emphasis on smoking status. As opposite results, they cited one report of positive association between smoking and depression both in men and women with the mean age (one standard deviation) of 49.2 (10.6) in men and 50.8 (12.8) in women, respectively.2
Luger et al.3 conducted a systematic review by meta-analyses to know the association between smoking and depression. Both in cross-sectional and prospective studies, current smokers have a risk of depression against never smokers or former smokers by adjusting age. Tjora et al.4 also reported a prospective study on the association between smoking and depression from adolescence to adulthood, concluded that the relationship was established in early adolescence and maintained into adulthood. They collected 924 adolescents and followed them until the target subjects became 30 years old.
I present here the level of depression by splitting subjects into several age classes and smoking status from a cross-sectional study, which confirmed that the association between smoking status and depression was observed only in young generation.
The study participants consisted of 3183 male workers of a Japanese railway company, aged from 25 to 54 years old. Individuals with prior diagnosis of severe depression were excluded. Informed consent was obtained from each of the participants prior to their enrollment in the study, and the study was approved by the railway company. Age and smoking status (no, past, current) were asked by questionnaire.
Participants also completed the Zung Self-Rating Depression Scale (SDS), a clinical screening tool for depression. The SDS is a 20-item self-rating instrument that was designed by Zung et al.5 Responses are given on a four-point Likert-type scale, wherein each item is scored from 1 (never) to 4 (extremely). The raw score, which ranges from a minimum of 20 to a maximum of 80, is obtained by adding the scores for the 20 responses. An Index score (SDSI), ranging from a minimum of 25 to a maximum of 100, is derived by multiplying the raw score by 1.25. Jegede noted that the SDS shows internal consistency reliability (Cronbach's alpha coefficient=0.75) and construct validity (average item-correlations=0.36).6 The sensitivity and specificity of SDS as a screening tool for DIS/DSM-III depression in non-psychiatric outpatients have been reported to be 97% and 63%, respectively.7 No information on antidepressant treatment could be obtained from the patients.
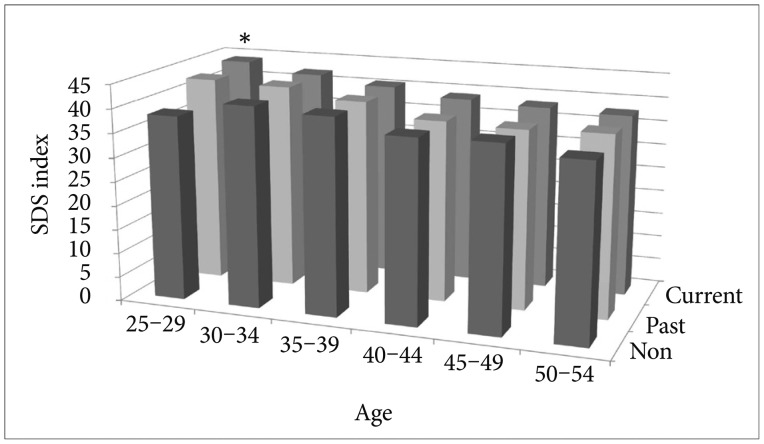
Mean values of SDSI, stratified by age class and smoking status, were presented in Figure 1. Significant difference in the mean value between non-smokers and current smokers was only recognized in subjects, aged from 25 to 29 years old. Thereafter, significance disappeared among smoking status in each age class.
From this study, the association between smoking and depression seems to be recognized in subjects under 30 years old. Noh et al. handled subjects aged 45 or older, and their study outcome was in concordance with my study. Further study is needed for trend analysis with different ethnicity, gender, lifestyles and depression measurement methods.