INTRODUCTION
In 2013, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) of the American Psychiatric Association included Internet Gaming Disorder (IGD) in Section III, thus warranting more research before it might gain official recognition.1
According to recent studies,2 researchers discussed the addition of non-substance-related addictive disorders to DSM-5. IGD was added based upon reviews, a voting process, about 250 research publications, and from the growing medical risk of IGD.
There are several difficulties in properly diagnosing and treating IGD. While the number of publications related to 'internet game addiction',345 'internet game dependency',678 'IGD',291011121314 and other names1114 has been steadily on the rise, the consensus on the standards of IGD has not yet been reached. Therefore, concept of IGD needs to be clarified further and standardized criteria for research has to be developed.
Research on IGD prevalence7151617181920 has shown limited consistency. Depending on the criteria used, prevalence rates vary from less than 1%151617 to approximately 10%2181920 In addition, many reports focus on children, adolescents, and young adults, resulting in a general lack of adult-targeted research.
To address the efficacy of the IGD classification of DSM-512 and the limited consensus on the proposed criteria,1 the appropriateness of the proposed diagnostic criteria of DSM-5 should be examined systematically. To this end, studies to develop standardized and refined criteria and integrated assessment methods are necessary.2
This study aimed to characterize different psychiatric symptoms of IGD, including internet gaming experience, motivation and impulsivity by comparing the risk group and healthy control group applying DSM-5 diagnostic criteria as an extension of an international collaborative research effort involving eight countries (including for example, Korea, Hungary, and the United Kingdom). Secondly, we also aimed to estimate IGD prevalence among adults in Korea.
METHODS
Cross-cultural data collection and questionnaire translation
The same online questionnaire was used to collect data from gamers speaking Hungarian, English, Italian, Norwegian, Slovenian, French, Romanian, and Korean. For the Korean survey, however, we included additional questions pertaining to the DSM-5 diagnostic criteria in order to derive the estimation of adult IGD Characteristics.
Translations of the survey were carried out by research colleagues from the respective collaborating countries and back translated by another expert. The back-translations of the initial Korean version of the survey were compared with the original English version and differences were discussed until a consensus was reached by a graduate-level bilingual. The final version was shown to a group of gamers who gave their opinions regarding the clarity and comprehension of the items.
Subjects
A total of 3041 adults (20 to 49 years of age) who had engaged in Internet gaming within 6 months from the start of the study participated (data collected from March 17-28, 2014). The data collection was carried out by Korea's Most Prestigious Market and Opinion Research Firm (KMPMORF) through the Computer Aided Web Interview (CAWI) method. The informed consent was obtained from participants prior to their inclusion in the survey. This study was approved by the Institutional Review Board of the Eötvös Loránd University in Hungary and Eulji University in Korea, respectively. The sample was not nationally representative. The survey was completed through random in Korea. Total sample size was 3041 (Men n=1824, Women n=1217).
Measurements
Sociodemographic data
Major sociodemographic characteristics such as gender, age, marital status, educational level, and current work status were obtained.
Gaming-related questions
Gaming-related questions such as online game type preference and weekly playing time were given. Based on previous findings,21 three popular game types [first-person shooter (FPS), role playing games (RPGs), and real time strategy (RTS) games] and an 'other' categories were offered to identify main game type preference.
Categories for weekly playing time were the following: less than 1 hour a day (less than seven hours weekly), 1-2 hours per day (7-14 hours weekly), 2-4 hours per day (15-28 hours weekly), 4-6 hours per day (29-42 hours weekly), and more than 6 hours per day (more than 42 hours weekly).
The Motives for Online Gaming Questionnaire22 (MOGQ)
MOGQ is a 27-item self-reported questionnaire assessing the full range of motives for online gaming, including escape (4 items), coping (4 items), fantasy (4 items), skill development (4 items), recreation (3 items), competition (4 items), and social (4 items). The instrument uses a 5-point Likert scale from "never" to "almost always/always," with higher scores indicating higher frequency of the respective motivational dimension. Internal consistencies were reported for all seven dimensions, ranging from 0.79 to 0.9022 and the present sample as well (Cronbach's alpha=0.912).
The diagnostic criteria of IGD in DSM-5
In DSM-5, IGD is identified in section III as a condition warranting more clinical research and experience before it might be considered for inclusion in the main book as a formal disorder. The diagnostic criteria of IGD in the DSM-5 are composed of 9 items: preoccupation, withdrawal, tolerance, unsuccessful attempts to control, loss of other interests, continued excessive use despite psychosocial problems, deceiving regarding online gaming, escape, and functional impairment1. Meeting five or more DSM-5 criteria of IGD proved to be the best cut-off point in a previous study.11 The suggested wordings of the DSM-5 criteria was applied in this computer aided web interview using a "yes" or "no" response form. According to these DSM-5 criteria, we divided the participants into risk group and healthy controls. We used the term 'risk group', not 'patient group', because we did not confirm the diagnosis with clinical interview.
BSI2324252627
To assess self-reported clinically relevant psychological symptoms and distress, the present study used the Brief Symptom Inventory (BSI).24 This 53-item questionnaire uses a 5-point Likert scale (from "not at all" to "extremely") and comprises nine symptom dimensions: somatization (7 items), obsession-compulsion (6 items), interpersonal sensitivity (4 items), depression (6 items), anxiety (6 items), hostility (5 items), phobic anxiety (5 items), paranoid ideation (5 items), and psychoticism (5 items). Good reliability and validity have been found across various samples232428 and the present sample as well (Cronbach's alpha=0.982).
BIS29
Impulsivity was measured by the 21-item revised version of the original Barratt Impulsiveness Scale (BIS).29 The 21 items comprise three factors [self-control (9 items), impulsive behavior (5 items), and impatience (7 items)] and the factors are rated on a 4-point Likert scale (from "rarely/never" to "almost always/always"). The Cronbach's alpha of present sample was 0.769.
Statistical analysis
All analyses were conducted with SPSS software version 18.0 (SPSS, IBM corp., NY, USA). A p level lower than 0.05 was considered significant. Prevalence was derived based on the percentage of participants giving positive responses to five or more DSM-5 criteria of IGD as suggested by previous clinical research.1211
Further, we analyzed the differences between the healthy control and risk group in order to investigate the sociodemo-graphic characteristics, and psychiatric symptoms associated with internet game overuse.
The descriptive data were expressed as frequency and percentage or mean and standard deviation. Chi-square analyses and analysis of variance (ANOVA) were used to test the difference of distribution, and the mean differences between the healthy control and risk group. Lastly, to investigate the relationship among variables in the diagnosis of IGD, the Pearson's correlation coefficient was used.
RESULTS
Sociodemographic characteristics
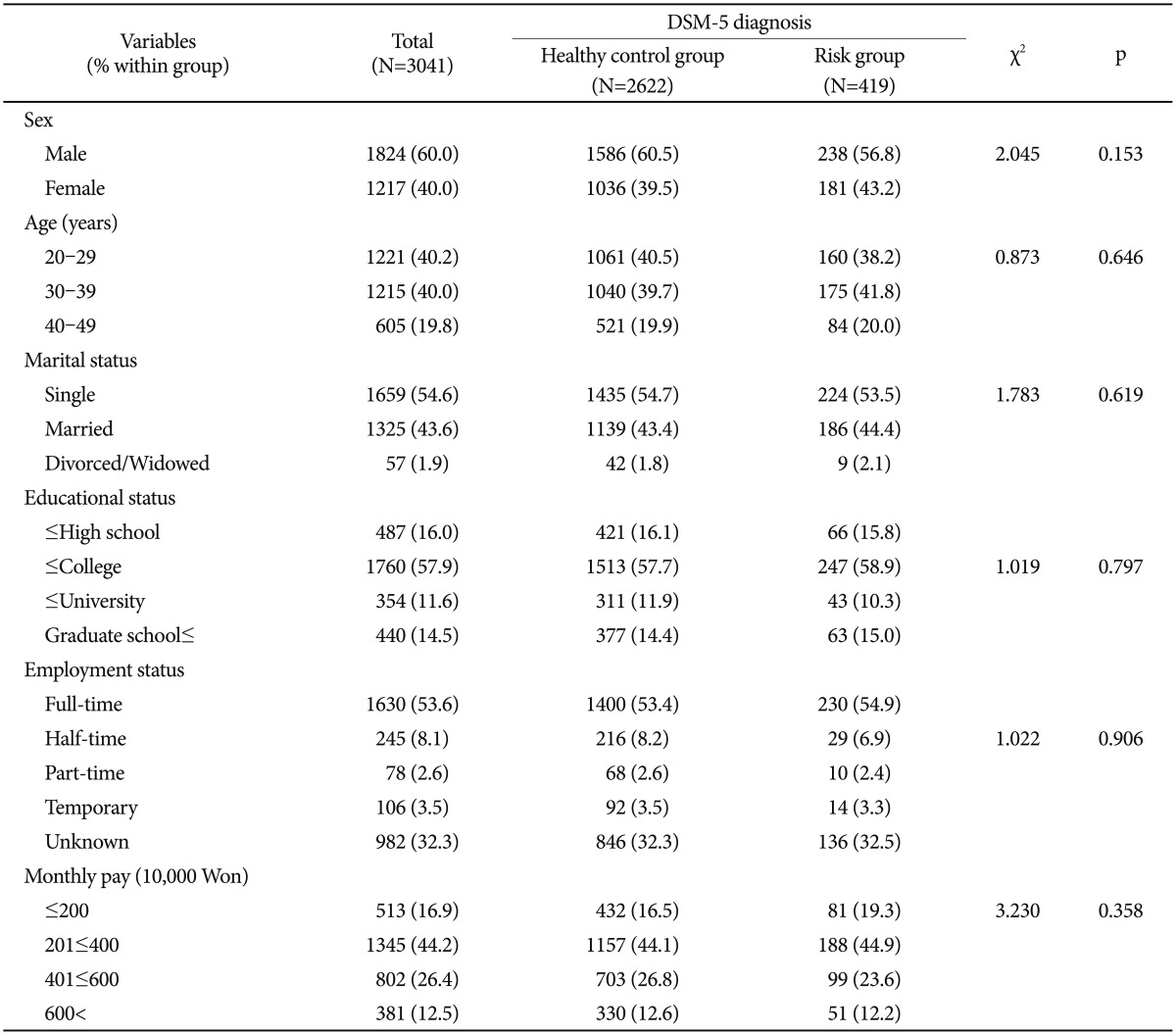
Among the 3041 participants, 419 subjects (13.8%) were identified and labeled as the IGD risk group and 2622 subjects (86.2%) were labeled as healthy controls (Table 1). The frequency of men (60.0%) was higher than that of women (40.0%), and most individuals were in their twenties to thirties, accounting for 80.2% of participants. Most were single (54.6%), followed by married (43.6%) individuals. Most had not graduated college (57.9%) and held a full-time job (56.3%). In-come levels show that the highest proportion (44.2%) of people earned monthly income between 2,000,000 and 4,000,000 won (approximately 1800-3600 USD).
Online-game playing time
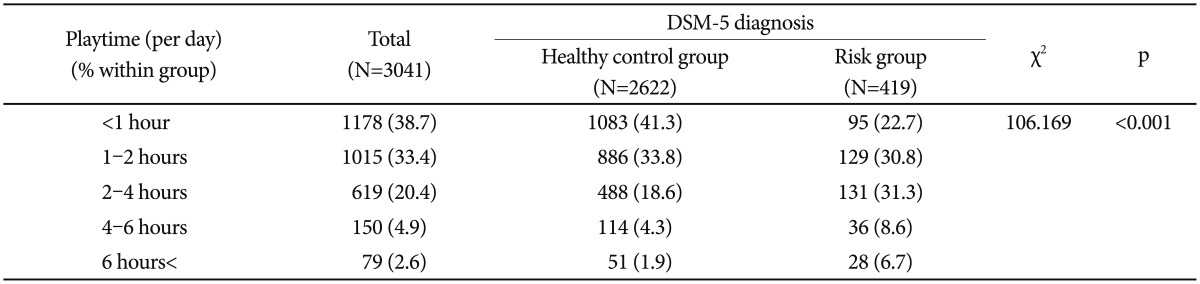
The online-game playing time is shown in Table 2. Most individuals played less than 1 hour a day (less than 7 hours weekly) (38.7%), followed by 1-2 hours per day (7-14 hours weekly) (33.4%), 2-4 hours per day (15-28 hours weekly) (20.4%), 4-6 hours per day (29-42 hours weekly) (4.9%), and more than 6 hours per day (more than 42 hours weekly) (2.6%). The risk group subjects tended to belong significantly more to the categories with a relatively high weekly online game playtime than healthy controls (p<0.001).
Online-game type
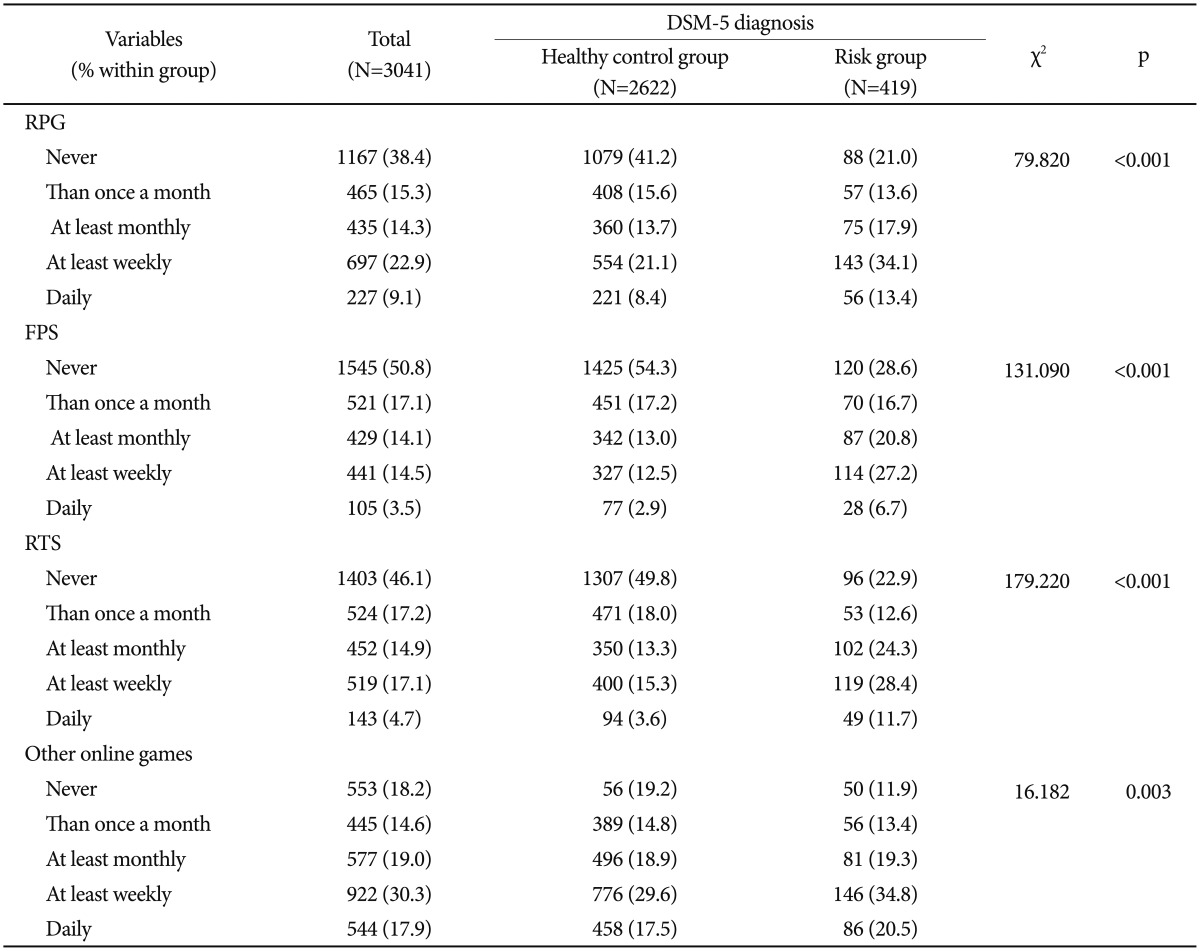
On average, 22.9% of subjects played RPGs at least once a week, and 9.1% played them every day (Table 3). The frequency of RPG use in the risk group was on average about 1.6 times higher than for healthy controls (p<0.001). In the case of FPS games, 14.5% played at least once a week on average, and 3.5% played every day. The FPS games were played by the risk group approximately 2 times more frequently than by healthy controls (p<0.001). For RTS games, 17.1% of subjects played at least once a week on average, and 4.7% played every day. The frequency of RTS game play in the risk group was on average about 2 times higher than in the case of healthy controls (p<0.001). The frequency of 'other' online games (sports, puzzle, etc.) was about 1.2 times higher in the risk group as compared with healthy controls (p<0.003). On average 30.3% played 'other' games at least once a week, and 17.9% played them every day.
The motives for online gaming
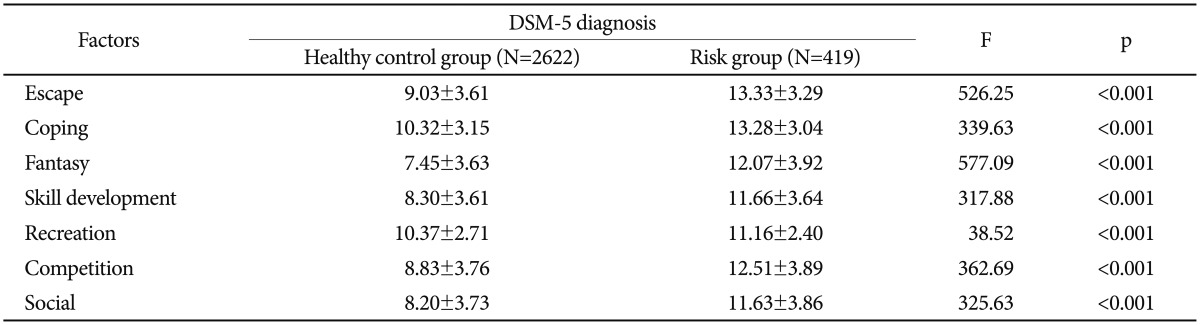
Using the MOGQ to assess the motives for online gaming, the risk group used online gaming to escape from reality or specific issues more than the healthy controls (13.33 vs. 9.03, p<0.001, respectively) (Table 4). Also, the risk group showed higher score in the use of online gaming as a coping mechanism compared to the healthy control group (13.28 vs. 10.32, p<0.001, respectively). Likewise, the risk group scored significantly higher on all other motivation subscales (12.07/7.45, 11.66/8.30, 0.16/10.3711, 12.51/8.83, and 11.63/8.20 for fantasy, skill development, recreation, competition, and social, respectively, p<0.001).
Correlation between online game types and the motives for online game
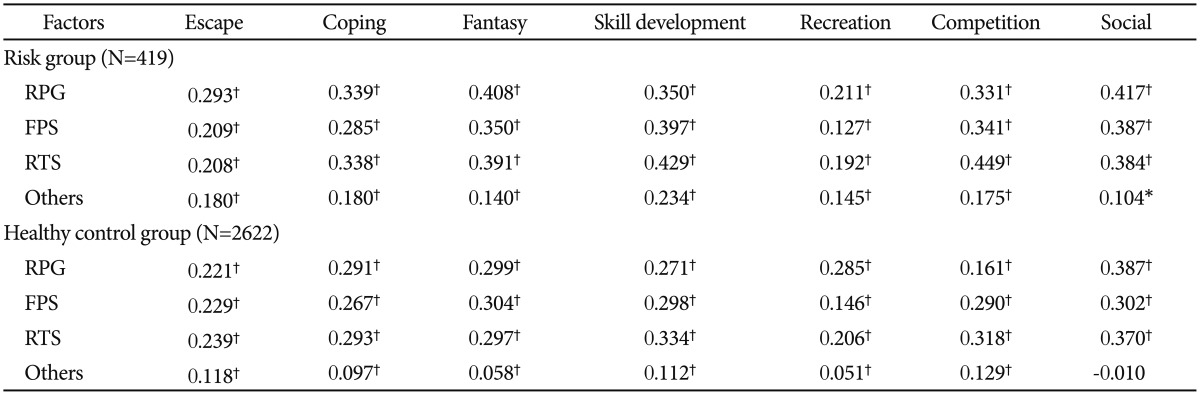
Table 5 shows the correlations between online game type by subjects and the motives for online game play (MOGQ). The seven motivation factors for online gaming were positively correlated with the game type choice for individuals in the risk group. The range of correlations between game type and MOGQ was 0.104-0.449.
The use of RPGs by subjects of the IGD risk group was strongly correlated with fantasy (r=0.408, p<0.01) and social (r=0.417, p<0.01) factors. FPSs users in the IGD risk group were significantly correlated with skill development (r=0.397, p<0.01), and RTS game users in the IGD risk group were significantly correlated with both skill development (r=0.429, p<0.01) and competition (r=0.449, p<0.01).
The use of RPGs and RTS games by healthy controls were significantly correlated with social factors (RPGs: r=0.387, p<0.01; RTS: r=0.370, p<0.01, respectively). FPSs healthy control use was significantly correlated with fantasy (r=0.304, p<0.01) and social (r=0.302, p<0.01) factors as the motives to play online games.
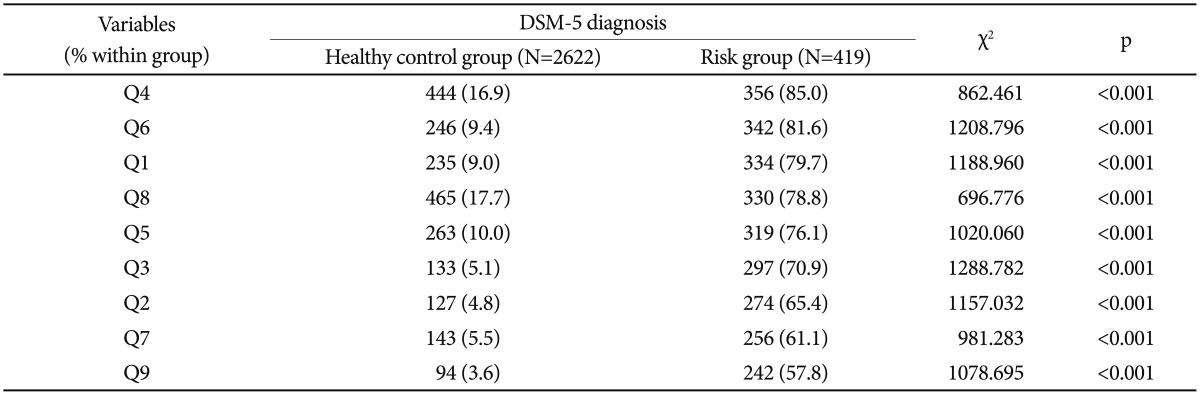
Difference between the healthy control and risk group in the nine proposed DSM-5 diagnostic criteria
The risk group showed higher frequency of endorsement of all nine DSM-5 diagnostic criteria compared to the healthy control group. The results are presented in Table 6.
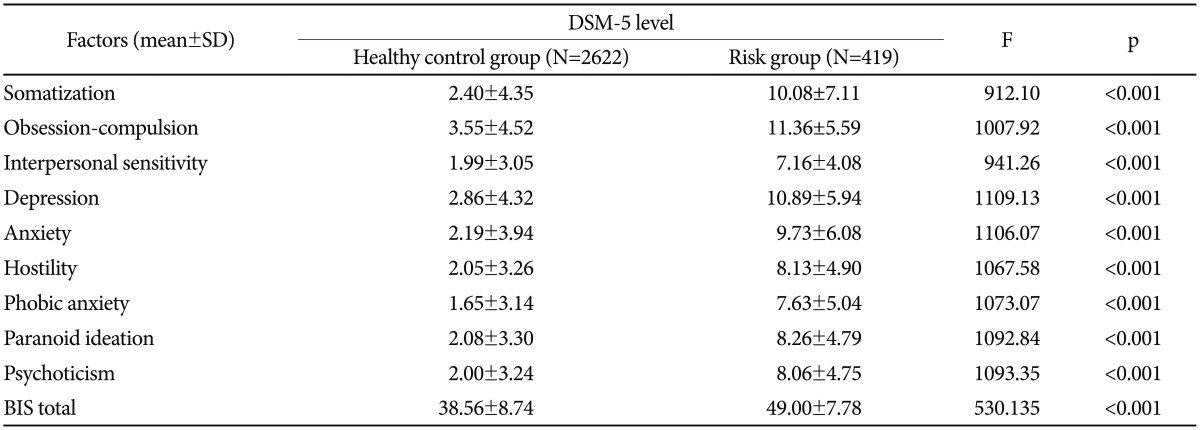
Psychiatric symptoms & impulsivity
The BSI and BIS were used to assess the symptoms related to IGD. The mean scores of the risk group were noted to be significantly higher than those of healthy controls (Table 7). 'Obsession-compulsion', 'depression', and 'somatization' symptoms of the BSI were markedly higher in risk subjects than in the healthy control subjects, and the total BIS scores related to impulsivity were higher in the risk group as well.
DISCUSSION
This report presents the prevalence and symptoms of IGD as measured by an online survey of adults who engaged in recent Internet gaming. It was based on self-reported data on the criteria listed in the DSM-5. DSM-5 section III highlights the need for further investigation on IGD, and has proposed nine diagnostic criteria as suitable tools for IGD diagnosis. Applying the 5 cut-off point criteria as based on major preceding research21011 and as suggested by the DSM-5, 13.8% of all participants were categorized into the at-risk IGD group. Approximately 7.4% of adults aged 20-40 years were determined to be in the IGD risk group in our study, taking into account that 53.4% of this age group plays online games, as surveyed by the National Information Society Agency in Korea.30 In Germany, a study by Festl et al.15 showed a prevalence of 3.7% in adolescents and adults. In addition, Ferguson and colleagues reported the prevalence of IGD in the United States to be 3.1% in a meta-analysis of 33 published studies.17 In light of these data, the prevalence rate appears to be higher in Korea. In these studies, the disparity among the prevalence rates seems to be attributable to a number of factors, such as Internet environment, participants, diagnostic criteria, research methods, research period, and culture.
In this study, the difference in sociodemographic variables were not statistically significant between the healthy controls and the risk group. Therefore, sociodemographic variables do not appear to be significant factors in IGD diagnosis.
The risk group subjects tended to belong significantly more to the categories with a relatively high weekly online game playtime than healthy controls. However, in the risk group, almost all subjects belonged to the categories with a relatively low weekly online game playtime (<1 hour: 22.7%, <4 hour: 84.8%). This is because DSM-5 criteria do not have the concept of exact game playtime. Our results are merely a clinical reference, and did not show the importance of game playtime in IGD, exactly. Therefore, we think that more detailed and systematic studies on the relationship between IGD and game playtime are needed.
In the assessment of motivations for online gaming, all factors measured in the MOGQ were significantly higher in the risk group; the primary motivations (those with the highest scores) for online gaming were 'escape' and 'coping'. To our best knowledge, there has not been a comprehensive study on the IGD in adults based on MOGQ. One study31 of adolescents using the Internet Motive Questionnaire for Adolescents (IMG-A) demonstrated that 'coping' was a major motivation for online gaming use in subjects diagnosed with IGD. In addition, one study32 for pathological use of Internet games among Korean adolescents using the Internet Game Addiction (IGA) showed that 'escape' from self best explained the IGD. These results are in agreement with the data from this study.
Correlation analysis between online game types and the motives for online gaming revealed that there is a difference in the motives according to online game types between the risk group and healthy controls. In healthy controls, the motive for online game use strongly correlated with 'social' motivation regardless of the game type. On the other hand, the motives for online game use in risk individuals appeared to be different according to characteristics of each game type. These results suggest that risk subjects have more various motives for online game use than healthy controls, and have tendency to select game type by motives.
A positive response to the nine symptoms delineated in the DSM-5 diagnostic criteria of IGD was significantly higher in the risk group. This study found the DSM-5 criteria well identified the risk group.
The risk group scores were significantly higher in the factors of the BSI and BIS related to pathologic internet gaming use. The results show that the IGD risk group experienced more episodes of difficulty concentrating, loneliness, and insomnia. The risk subjects were also five times more likely to attempt suicide, be impulsive, and exhibit aggression than the healthy control group (p<0.001). These results are consistent with existing research333343536 on the relationship between psychiatric symptoms and disordered internet use which most studies have focused on thus far. Therefore comparison between our results and those of previous research should be done with caution. Nonetheless, this research may serve as a basis for developing prevention strategies, education, and therapeutic interventions for IGD to include adult population.
There are some limitations of this study. First, the sample of our study may not be considered as representative of the Korean population as a whole. The results of our study are also limited in its generalizability to other countries. Second, the diagnostic criteria of IGD in DSM-5 used in this study were not standardized and were based upon self-reporting; therefore, we did not confirm the diagnostic criteria with clinical interview. In addition, all other survey tool including psy-chometric questionnaire was also based upon self-reporting. However, it is important to note that DSM-5 diagnostic criteria were applied to a large number of adult individuals rather than children and adolescents. In addition, this study examined the various psychopathological aspects using scales and provided important baseline data and evidences supporting the suggestions for the IGD diagnostic criteria of the DSM-5. Future studies should attempt to overcome the limitations of this paper with respect to the sociodemographic background and environment of subjects and seek further validation of our results with clinical diagnostic interviews.