INTRODUCTION
The suicide rate in South Korea increased to 31.2 per 100,000 persons in 2008 from 15 per 100,000 persons in 1999.12 Thus, public concerns about suicide risk and prevention have increased.
It has been reported that suicide is strongly associated with suicidal ideation and attempts,3 and mood disorders, substance disorders, and schizophrenia have been established as risk factors for suicidal behaviors.4567
Weissman et al.8 published a seminal article suggesting that panic disorder had a stronger association with suicide attempts compared to the general population (OR=17.99, 95% CI: 12.18-26.58) based on more than 18,000 adults living in the community. Subsequently, many studies reported that anxiety disorders, including panic disorder, were associated with suicide ideation and suicide attempts,910 although there were inconsistent results and controversies.11 An overactivate hypothalamus-pituitary-adrenal HPA axis coupled with anxiety is one of the contributing factors for suicide.12 However, anxiety disorder and related neuroendocrinological dysregulation alone might not directly cause the completed suicide. It has been suggested that comorbidity should be considered when evaluating risk factors for suicidal behaviors because psychiatric disorders can occur concurrently.13 Sareen14 argued that the controversy regarding associations between anxiety disorders and suicidal behaviors may be attributable to differences in the methods used to adjust for comorbid non-anxiety mental disorders. Accordingly, statistical analyses should control for each mental disorder separately.
To date, few studies using nationally representative community samples have examined whether individual anxiety disorders are associated with suicidal behavior after adjusting for other mental disorders.
Therefore, we aimed to examine the association between lifetime histories of individual anxiety disorders and lifetime histories of suicidal behavior while adjusting for sociodemographic factors, mood disorders, alcohol use disorders, and psychotic disorders.
METHODS
Participants
Data for this study were obtained from The Korean Epidemiologic Catchment Area Study-Replication (KECA-R),15 which was based on a stratified multistage area probability sample of the non-institutionalized South Korean population aged 18-64 years. The response rate for the study was 81.7%. The Institutional Review Board of the Seoul National University College of Medicine approved this study. All subjects were fully informed about the aims and methods of the study before the interview was conducted. Informed consent was obtained prior to participation. Detailed descriptions of the sampling procedures have been reported previously.15
Sociodemographic information including sex, age, cohabitation status, and education was obtained at the time of enrolment.
Assessment of lifetime DSM-IV psychiatric disorders
Each participant was assessed in person by a trained interviewer based on the Korean version of the Composite International Diagnostic Interview (K-CIDI),16 a fully structured, lay-administered diagnostic interview designed to identify psychiatric diagnoses according DSM-IV criteria.17 The K-CIDI was previously validated by Cho et al.18 according to the World Health Organization guidelines.19 This study assessed the lifetime prevalence of the following DSM-IV psychiatric diagnoses using the K-CIDI: agoraphobia without panic disorder, generalized anxiety disorder (GAD), panic disorder without agoraphobia, post-traumatic stress disorder (PTSD), specific phobia, social phobia, obsessive-compulsive disorder (OCD), major depressive disorder, dysthymia, bipolar disorder, alcohol abuse or dependence, and psychotic disorders.
Lifetime suicidal ideation, plan, and suicide attempts
Respondents' histories of suicidal ideation and suicide attempts were assessed during the life-event history section of the interview based on the following questions. The suicidal ideation question was ‘Have you ever seriously thought about committing suicide?’. The suicidal plan was measured by a question ‘Have you ever concretely planned suicide?’ Suicidal attempt was measured by the following question, ‘Have you ever attempted suicide?’ We further used following questions to differentiate suicidal attempt from suicidal gesture or self-harming behaviors: 1) I made a serious attempt to kill myself and it was only luck that I did not succeed. 2) I tried to kill myself but I knew the method was not fool-proof. 3) My attempt was a cry for help. I did not want to die. According to the previous studies,2021 we only defined 1) and 2) as suicide attempt. Responding to 3) was defined as a suicidal gesture. Respondents who answered in the affirmative with regard to suicidal ideation (n=1005), plan (n=225), or suicide attempts (n=166) were included in the analysis.
Statistical analysis
Cohabitation status was divided into two categories: cohabitation and living alone. Age and education were treated as continuous variables. Univariate logistic regression analyses were used to examine the relationship of lifetime suicidal ideation and suicide attempts with demographic variables and lifetime DSM-IV psychiatric diagnoses, including anxiety disorders. Next, multiple logistic regression analyses were performed using variables found to be associated with suicidal ideation, suicidal plan, suicide attempts, and major depressive disorder (MDD) in the univariate logistic regression analyses. The multiple logistic regression analyses treated lifetime diagnoses of anxiety disorders (agoraphobia, GAD, panic disorder, PTSD, specific phobia, social phobia, and OCD) as independent variables. Covariates in the analysis were sex, age, education, cohabitation status, lifetime diagnosis of MDD, dysthymia, bipolar disorder, alcohol abuse or dependence, and psychotic disorders. When the MDD was set as a dependent variable, covariates were sex, age, education, cohabitation status, lifetime diagnosis of dysthymia, bipolar disorder, alcohol abuse or dependence, and psychotic disorders. Adjusted odds ratios (ORs) and 95% CIs were calculated based on these multiple logistic regression models. Statistical analyses were performed using SPSS software, version 16.0.
RESULTS
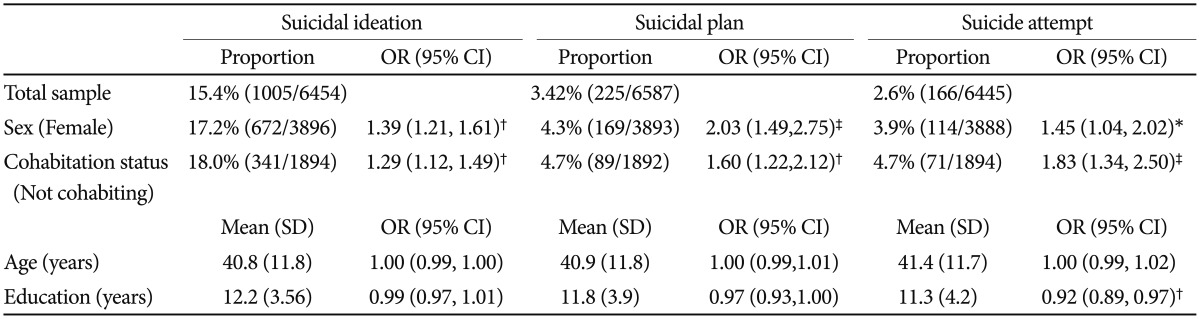
Table 1 presents the results of the univariate analysis of the association of lifetime suicidal ideation and suicide attempts with demographic variables. Being female (OR=1.39, 95% CI: 1.21-1.61; OR=1.45, 95% CI: 1.04-2.02) and living alone (OR=1.29, 95% CI: 1.12-1.49; OR=1.83, 95% CI: 1.34-2.50) were significantly associated with both suicidal ideation and suicide attempts. Associations of demographic variables, such as age and education, with suicidal ideation and suicide attempts were not significant with the exception of the correlation between education and suicide attempts (OR=0.92, 95% CI: 0.89-0.97).
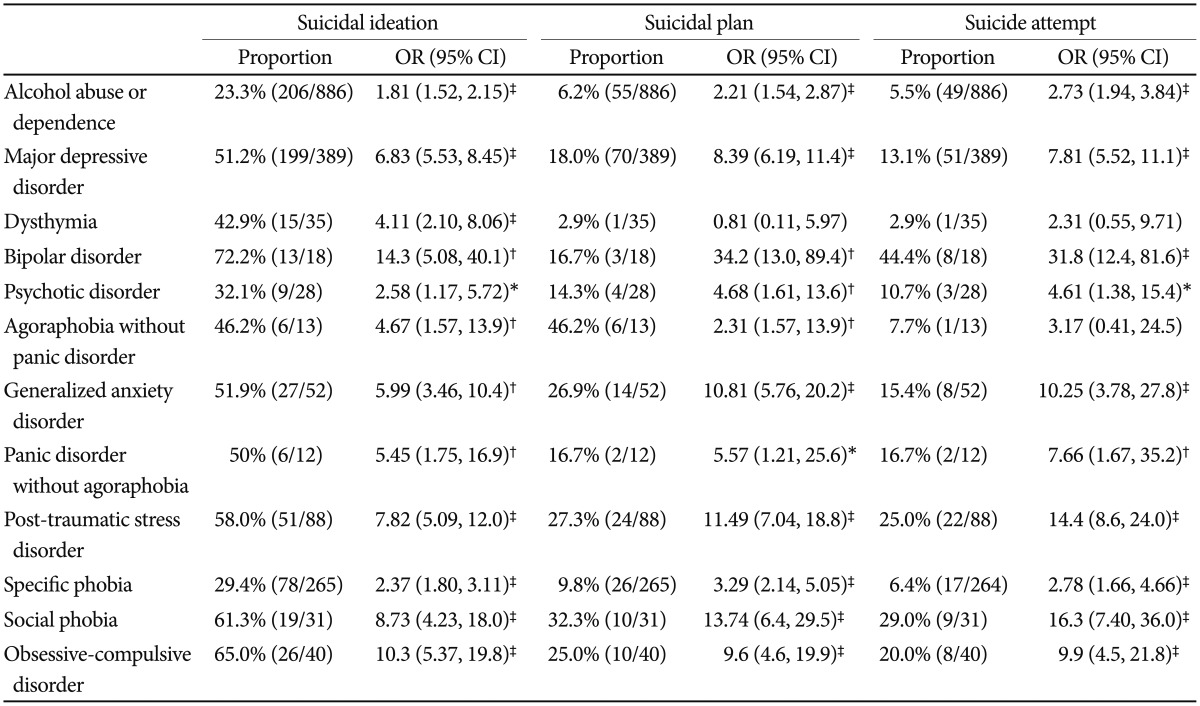
Table 2 presents the relationship of each psychiatric diagnosis with suicidal ideation and suicide attempts. All psychiatric disorders were significantly associated with suicidal ideation, and, with the exceptions of dysthymia (OR=2.31, 95% CI: 0.55-9.71) and agoraphobia without panic disorder (OR=3.17, 95% CI: 0.41-24.5), with suicide attempts.
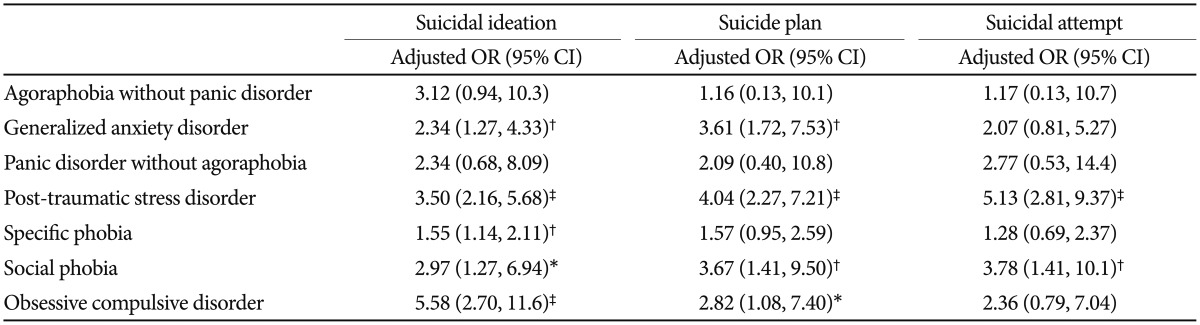
Table 3 presents the relationship of anxiety disorders with suicidal ideation and suicide attempts by psychiatric comorbidity and sociodemographic characteristics. GAD (OR=2.34, 95% CI: 1.27-4.33), PTSD (OR=3.50, 95% CI: 2.16-5.68), specific phobia (OR=1.55, 95% CI: 1.14-2.11), social phobia (OR=2.97, 95% CI: 1.27-6.94), and OCD (OR=5.58, 95% CI: 2.70-11.6) remained significantly associated with suicidal ideation. Agoraphobia without panic disorder (OR=3.12, 95% CI: 0.94-10.3) and panic disorder without agoraphobia (OR=2.34, 95% CI: 0.68-8.09) were no longer significantly associated with suicidal ideation. Social phobia (OR=3.78, 95% CI: 1.41-10.1) and PTSD (OR=5.13, 95% CI: 2.81-9.37) remained significantly associated with suicide attempts, whereas panic disorder without agoraphobia (OR=2.77, 95% CI: 0.53-14.4), specific phobia (OR=1.28, 95% CI: 0.69-2.37), GAD (OR=2.07, 95% CI: 0.81-5.27), and OCD (OR=2.36, 95% CI: 0.79-7.04) did not.
Table 4 presented the relationship of anxiety disorders with MDD. Among anxiety disorders, GAD (OR=10.24, 95% CI: 5.59-18.75) had the highest association with MDD, followed by panic disorder (OR=7.82, 95% CI: 2.31-26.55), social phobia (OR=7.00, 95% CI:3.03-16.16), and PTSD (OR=4.48, 95% CI: 2.69-7.48). Agoraphobia (OR=2.09, 95% CI: 0.34-12.73) was the only anxiety disorder which was had no association with MDD.
DISCUSSION
This is the first epidemiological study to investigate the relationship between DSM-IV anxiety disorders and suicidal behavior using a nationally representative South Korean sample.
The findings of this study suggest that GAD, PTSD, social phobia, specific phobia, and OCD are independent risk factors for suicidal ideation, whereas only PTSD and social phobia are predictors of suicide attempts. Panic disorder and agoraphobia were not associated with suicidal ideation, plan, and attempt. These results were obtained after adjusting for other important variables, including major DSM-IV axis I disorders and sociodemographic variables including age, sex, cohabitation status, and education.
Particularly, statistical significance of the influence of PTSD increased with the degree of suicidality. Adjusted OR of PTSD for suicidal idea, suicidal plan, and suicidal attempt were 3.50, 4.04, and 5.13, respectively. These results suggested that the proclivity of PTSD for suicide is the severest among anxiety disorders. Several studies have consistently reported that patients with PTSD have high rates of suicidality.22 Our findings were similar to previous studies, in which PTSD was commonly correlated with suicidal attempts.2324 Although the impact of individual anxiety disorders for suicide risk has been addressed by previous studies, many studies focused on PTSD alone, or other anxiety disorders excluding PTSD.25 However, our study measured all sort of anxiety disorders, which is the principal difference with the previous studies.
There have been inconsistent results concerning social phobia. Whereas we showed that social phobia is associated with suicidal ideation, plan, and attempt, Schneider et al.26 found that social phobia was associated with suicidal ideation but not with suicide attempts. These differences may be attributable, in part, to the fact that that study included variables coded for three and more lifetime DSM-III-R disorders and included antisocial personality disorder in the multivariate logistic regression analysis, which may have reduced the significance of some predictors of suicidal behaviors.
GAD and OCD were associated with suicidal ideation and plan, but not with suicidal attempts. Previous studies have consistently found that patients with GAD, one of the most common mental illnesses, with a lifetime prevalence of more than 5%,27 had higher suicidality than did those without GAD.2829 A previous Chinese study reported that 37.6% of patients with a lifetime history of GAD had a history of suicide attempts, whereas only 4.2% of those without GAD had such a history.29 A study conducted in Europe also reported that suicide attempts and suicidal ideation were more frequent in patients with GAD than in those without.28 Regarding suicidal risk of OCD, Sareen et al.30 found that social phobia and OCD were associated with suicidal ideation but not with suicide attempts. However, the Epidemiological Catchment Area Study found that OCD with or without a lifetime history of any other psychiatric disorder was associated with suicide attempts.31 Possible reason for the differential association between anxiety disorders (GAD and OCD) and suicidal behaviors (suicidal idea and suicide attempt) may result from the comorbid psychiatric disorders. Sareen et al.30 proposed that these anxiety disorders may have different relationships with suicidal behavior; that is, suicidal ideation may be directly related to social phobia and OCD, whereas suicidal attempt may be indirectly related and mediated by comorbid psychiatric disorders (depression, substance abuse, etc.). Since our study controlled possible influences of comorbid psychiatric disorders, thereby blocking the indirect pathway, GAD and OCD were not associated with suicide attempt. In OCD, clinical symptomatology might have influences on the suicidal behavior. For example, Kamath et al.32 reported that religion, reassurance seeking, and the repetitive symptoms of OCD were associated with suicide attempts.
Results from the current study differed from the results of previous studies that found panic disorder to be associated with suicidal ideation and suicide attempts.81123 The association of panic disorder with suicidality has been a recent focus, since it is assumed likely that patients with panic disorder have a fear of death, which would prevent them from committing suicide. Although comorbidity of panic disorder may play an important role for suicidal risk, there have been inconsistent conclusions on whether panic disorder independently increased suicidality.2333 Whereas panic disorder had no association with suicidality, it showed a close relationship with MDD. Following GAD, panic disorder was the second highest impacting anxiety disorder for the prevalence of MDD. Such observations were suggestive of different mechanisms of influence by anxiety disorder on suicide vs. depression. These considerations, which suggesting that comorbid psychiatric disorders have crucial role in the suicide attempt in anxiety disorders, may be applicable to the association between suicidal behaviors and specific phobia, in which only suicide idea was associated with specific phobia.
Our study has several notable limitations. First, we could not examine causal relationships between DSM-IV anxiety disorders and suicidal behavior, as this study used a cross-sectional design. Second, we assessed suicidality based solely on subjects'responses to the questionnaire and did not obtain confirmatory information. Third, because a number of psychiatric disorders have low 1-year prevalence, only lifetime prevalence rates were examined, which could have increased recall bias and further confused the causal relationships between suicidality and anxiety disorders. It is noteworthy that the prevalence of most of the DSM-IV psychiatric disorders were lower than those reported in other regions, despite the use of lifetime prevalence of anxiety disorders. For example, the prevalence rate of panic disorder without agoraphobia (0.19%) in South Korea was lower than the prevalence rate 3.7% in the United States.34 However, the suicide rate has been the highest in South Korea compared to other OECD countries.35 We surmised that the discrepancy between low psychiatric disorders and high suicide rates might be due to sociocultural factors such as stigma and prejudice. The fear of stigma might hinder the mentally ill from disclosing their psychiatric symptoms and seeking medical help. Several published findings have revealed the importance of socio-cultural factors, without a direct investigation on the relationship among stigma, psychiatric disorders, and suicide in South Korea. It has been reported that people living in regions with low suicide rates had less stigma associated with mental illness than regions with high suicide rates.36 Another study suggested that suicide rates were twice as high among South Korean emigrants in Japan than non-emigrants, indicative of a strong association with prejudice and economic factors.37
In conclusion, our study revealed that anxiety disorders, except for panic disorder and agoraphobia, were associated with suicidal ideation and plan. PTSD was the most influential factor for suicide attempt on adjusting for sociodemographic variables and other anxiety disorders. Future studies are necessary to identify psychosocial and neurobiological mechanisms underlying the suicidality of anxiety disorders. Cumulative effects of prior suicide attempts, comorbidity, and clinical characteristics of individual anxiety disorders should also be considered.