INTRODUCTION
Several psychiatric disorders have long been defined as psychological reactions to traumatic or stressful event(s).1234567891011 In the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5), such disorders are categorized as ŌĆ£trauma and stressor related disordersŌĆØ.1 This category includes reactive attachment disorder, disinhibited social engagement disorders, posttraumatic stress disorder (PTSD), acute stress disorder, and adjustment disorder. The common etiologic factor between trauma and stressor related disorders is a causal relationship between negative life events and symptomatology-in other words, these disorders are a reaction to psychological distress. A relatively new stress-related diagnostic concept termed posttraumatic embitterment disorder (PTED) has emerged.1213 PTED is another clinically meaningful reactive disorder to a stressful life event; however, PTED has yet to be classified in the DSM-5.
PTED, which was first described by Linden in 2003,12 was initially defined as a mental state characterized by 1) prolonged feelings of embitterment 2) resulting from a direct psychological reaction to 3) an event that is believed and perceived as a violation of one's basic beliefs and values. PTED is comparable to PTSD in terms of its association with trauma. However, there are two key distinctions. While trauma related to PTSD is severe and catastrophic, trauma related to PTED is minor and related to common events.1314 Furthermore, notable PTSD-related emotional symptoms, such as hypervigilance and tension, are anxiety-focused, whereas the main emotional symptom of PTED is ŌĆ£embitterment.ŌĆØ1213
Embitterment refers to a persistent, psychological state that includes feeling let down, shamed, or as if one has been a failure. It also includes feelings of injustice and helplessness, along with the urge to fight back and an inability to identify proper goals.121314 This definition of embitterment is very similar to a core psychopathological concept of the Korean, culture-bound anger syndrome Hwa-byung, also known as fire-illness. ŌĆ£HwaŌĆØ in Hwa-byung means fire, and it symbolizes a complex psychological reaction to chronic, unsolved emotional stressors.15161718 Hwa-byung is closely akin to PTED in at least two ways. First, Hwa-byung also emerges from a negative life event.192021 Second, individuals with Hwa-byung predominantly feel affronted, aggrieved, outraged, disgraced, and helpless.1718 These emotions are closely related to the embitterment observed in PTED.
The present study investigated the diagnostic overlap between PTED and Hwa-byung. More specifically, the co-occurrence of PTED and Hwa-byung in the general population was examined. Additionally, depression, perceived stress, suicidality, and state-trait anger expression were compared between each disorder group and a corresponding non-diagnostic group. This study adds to our understanding of the commonalities and differences between these two stress-related diseases that have similar psychopathology.
METHODS
Participants
Participants were recruited from January 2014 to March 2015 via face-to-face interviews, distribution of brochures, print advertisement postings in public places, and direct contact through public speaking engagements. Seventy-one participants were recruited through direct advertisement via brochures handed out in the main street of city center, which is the city's principle commercial area. One hundred and three participants were recruited by direct advertisement through printed postings in the city's only university hospital, which is also its biggest. Sixty-eight participants were recruited through direct advertisement in one middle school and two high schools. Finally, seventy-three participants were recruited at two separate public speaking sessions.
Recruitment was done in one of five metropolitan cities in South Korea. This city contains large manufacturing facilities, many public institutes, and large farming areas and fisheries. This city is highly industrial and many people work in factories. Environmental problems from noise, crowding, and pollution from widespread industrial activity have caused chronic stress to the citizens of this locale. In addition, the recent economic downturn in South Korea may have increased the stress on the populace. All the above situations are considered predispositions for Hwa-byung. Seventy-one participants were recruited through direct advertisement via brochures handed out in the main street of city center, which is the city's principle commercial area. One hundred and three participants were recruited by direct advertisement through printed postings in the city's only university hospital, which is also its biggest. Sixty-eight participants were recruited through direct advertisement in one middle school and two high schools. Finally, seventy-three participants were recruited at two separate public speaking sessions.
Face-to-face interviews and short surveys were carried out to identify participants who met the inclusion and exclusion criteria. Inclusion criteria were as follows: 1) age 12 to 75 years, 2) no report of current psychiatric treatment, no report of history of documented chronic psychiatric disorders, no report of suspected psychiatric disorders, and no history of a psychiatry clinic visit at any time in their lifetime, 3) Korean as a native language, and 4) fluency in Korean. Exclusion criteria were: 1) any lifetime psychiatric history, 2) any cognitive impairment, and 3) any physical or medical condition that would make completing the study protocol difficult (e.g., limb handicap, etc.). Written informed consent was obtained from all participants. The University of Ulsan College of Medicine, Ulsan University Hospital Institutional Review Board approved the protocol, which was conducted in accordance with the Declaration of Helsinki.
PTED diagnostics
The Korean versions of a diagnostic core interview and algorithm for PTED were used to diagnose PTED. Diagnostics consisted of two categories: Criteria A (core criteria) and Criteria B (additional symptoms); the sensitivity and specificity of these criteria are 94% and 92%, respectively.22
Core PTED criteria consist of experiencing an event that led to a noticeable and persistent negative change in mental well-being, was unjust or unfair, and caused feelings of embitterment, rage, and helplessness. Core symptoms of any related psychological or mental problem (e.g., depression, anxiety) could not be present prior to the event.
Additional PTED symptoms included 1) repeated intrusive and incriminating thoughts about the event, 2) extremely negative feelings when reminded of the event, 3) the critical event or its originator causing feelings of helplessness and disempowerment, 4) a prevailing depressed mood since the critical event, and 5) the experience of a non-distressing mood when distracted. Four or more of these additional symptoms are needed for a PTED diagnosis, and the stress duration should be more than 6 months.
Hwa-byung diagnostics
Participants were also assessed on diagnostic criteria1718 for Hwa-byung. This also included a diagnostic interview scale.1718 The scale (Hwa-byung scale) was categorized via ŌĆ£AŌĆØ, ŌĆ£BŌĆØ, and ŌĆ£CŌĆØ symptoms. ŌĆ£AŌĆØ symptoms (6 items) are core Hwa-byung symptoms consisting of items related to subjective anger, ukwool/boon (feelings of injustice), expressed anger, heat sensation, hostility, and ŌĆ£HaanŌĆØ. ŌĆ£BŌĆØ symptoms (8 items) are somatic or behavioral and consist of items related to pushing-up from the lower abdomen leading to chest tightness, epigastric mass, respiratory stiffness, palpitations, dry mouth, sighs, racing thoughts, and pleading behaviors. ŌĆ£CŌĆØ symptoms (8 items) are additional symptoms that consist of items related to sadness, anxiety/agitation, guilt, sleep disturbances, headaches/bodily pain, anorexia, being easily frightened, and the impulse to rush out of the room. Each item is scored from 1 to 4. Scores range from 22 to 88.
Anger scale
The Korean version of the State-Trait Anger Expression Inventory (STAXI-K) was used to assess experienced and expressed anger.23 The original scale was developed by Spielberger24 and was translated into Korean in 1997.23 Each item is a statement people use to describe their emotions when feeling angry. The scale consists of 22 questions, and each item is assessed on a 4-point scale (1=no anger; 4=maximum anger). The items deal with the expression of anger (eleven items are ŌĆ£anger-outŌĆØ) and repression of anger (eleven items are ŌĆ£anger-inŌĆØ). The repression items were questions addressing efforts to turn anger inward. The expression items were questions addressing efforts to turn anger outward towards others.
Suicidal ideation
To assess suicidal ideation, participants were asked to complete Beck's Scale for Suicidal Ideation (SSI).25 This was originally a clinician-rated scale; the SSI was translated and transformed into a self-report scale by Shin et al.25 The SSI consists of 19 items scored on a 3-point Likert scale.26 The recommended cutoff value for the Korean SSI is Ōēź9 for adults, Ōēź14 for undergraduates, and Ōēź16 for high school students; the SSI has a Cronbach's ╬▒=0.97. The present study applied the cutoff value for high school students to middle school students given the lack of recommended cutoff values for this group.
Depression
Depression was measured via the Beck Depression Inventory (BDI), which is a commonly used scale. The BDI is a self-report measure consisting of 21 questions, with each item scored on a 4-point scale (0 to 3). Total scores range from 0 to 63. Higher scores indicate more severe depressive symptoms. The recommended cutoff value for the Korean version of the BDI is Ōēź16, which differentiates depressive from normal control groups. The BDI has a sensitivity of 77% and a specificity of 84%.
Current stress level
The 14-item Perceived Stress Scale27 was used to assess general stress experiences. Each item is scored on a 5-point Likert scale with scores ranging from 0 to 56. Higher scores indicate more severe perceived stress.
Statistical analyses
Fisher's exact tests were performed to compare the number of individuals with posttraumatic embitterment disorder and the number of individuals with Hwa-byung between both the depressive and non-depressive groups and between the suicidal and non-suicidal groups. Mann-Whitney U tests were performed to compare scores on the SSI, BDI, perceived stress, STAXI, and Hwa-byung scales between individuals with and without PTED. Similar analyses were performed to compare individuals with and without Hwa-byung.
RESULTS
Demographics
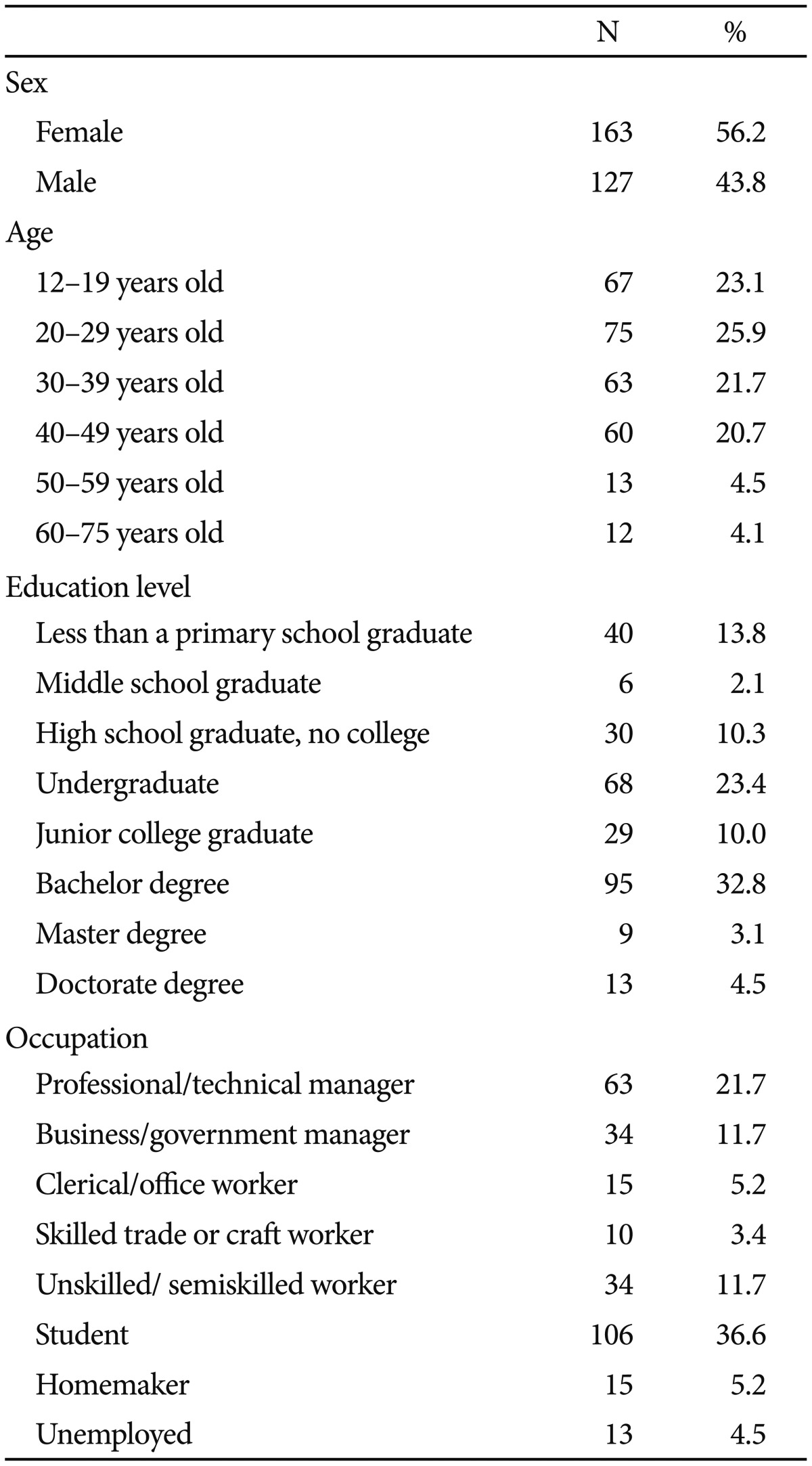
In total, 315 individuals satisfying both the inclusion and exclusion criteria consented to take part in this study. A total of 25 individuals with incomplete data were excluded. Analyses focused on the remaining 290 participants. Demographic data were obtained, including age, sex, education, and occupation (Table 1). The gender distribution was 127 males (43.8%) and 163 females (56.2%). Occupation categories were determined by following the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I). Mean participant age was 31.34 years (SD=13.33), and the mean years of education was 13.01 years (SD=3.45). Gender differences emerged for age, education, and occupation distributions. The female group was much younger (p<0.001) and less educated (p<0.001) than the male group. There were also more males than females working in the professional/technical and business/government management fields. Females were more predominant in the homemaker and student categories.
Among the 290 participants, 5 (1.7%; 4 females) were diagnosed with PTED and 6 (2.1%; 3 females) were diagnosed with Hwa-byung. There were no significant differences in the gender distribution for either PTED (p=0.39) or Hwa-byung (p=0.99) diagnoses. A representative case vignette for both PTED and Hwa-byung follows.
PTED
A 48-year-old man, previously employed as a factory worker, reported experiencing frequent outbursts of anger since suffering an injury at work about one year prior. The subject fell from a workplace about 5 m high and received multiple fractures of the ribs and spine. During his recovery, he has suffered from the memory of falling down and feelings of injustice towards his employer's irresponsible attitude. Six months post-injury, his application for an extension of worker's compensation insurance was rejected. He said that he felt deep embitterment towards society as a whole and he often feels like taking revenge on his employer and the staff of the worker's compensation insurance company. He spoke of these stories in a calm manner, despite nearly constant dysphoria since their occurrence. He has difficulties with concentration, sleep, and appetite.
Hwa-byung
A 60-year-old woman labeled herself as having ŌĆ£Hwa-byungŌĆØ. She has experienced frequent hot and burning sensation in the upper part of her body from the chest to head since learning of her husband's affair more than 30 years ago. When this sensation occurs, it begins in the chest and eventually spreads to the top of her head. When it is most severe, she feels a sensation reminiscent of someone pouring hot pepper on her chest, neck, and face. She has tried to cool down her body with air-conditioning, but it is useless. She has also experienced a feeling of something welling up in her throat. She designated her husband's repeated affairs as the cause of her symptoms. She has had to maintain her unwanted married life and endure this unfair situation for a long time due to considerations of her child and her lack of financial independence. She has felt angry and hateful to her husband for his unfaithfulness. She has also harbored feelings of bitterness and resentment towards a situation in which she has no way to revenge him and has no influence on her husband's behavior.
Associations of PTED and Hwa-byung with clinical scales
Scores on the SSI, PSS, BDI, and Hwa-byung scales were significantly higher among females than males (p<0.05). No differences were observed on the STAXI between females and males (p>0.05). When participants were divided into groups based on core and additional PTED diagnostic criteria, 6 participants met core criteria only and 28 met additional criteria only. The number of participants who met both criteria (core criteria and additional criteria) was 5. These 5 participants were diagnosed with PTED. No participant was diagnosed with both PTED and Hwa-byung. These results were replicated in a group that met sub-diagnostic criteria for PTED and the group diagnosed with Hwa-byung.
The percentage of individuals with higher suicidal ideation than normal was 10.1% (n=20), while the percentage of participants with more depressive symptoms than normal was 12.1% (n=25) (Table 2). However, neither the participants reporting high suicidal ideation nor those with depressive symptoms were diagnosed with PTED. Only one participant diagnosed with Hwa-byung was included in the higher suicidal ideation and depression group. There were no significant differences in suicidal ideation and depressive symptom scores between individuals with and without PTED. Additionally, there were no significant differences in diagnosed cases of suicidality and depression between individuals with and without Hwa-byung.
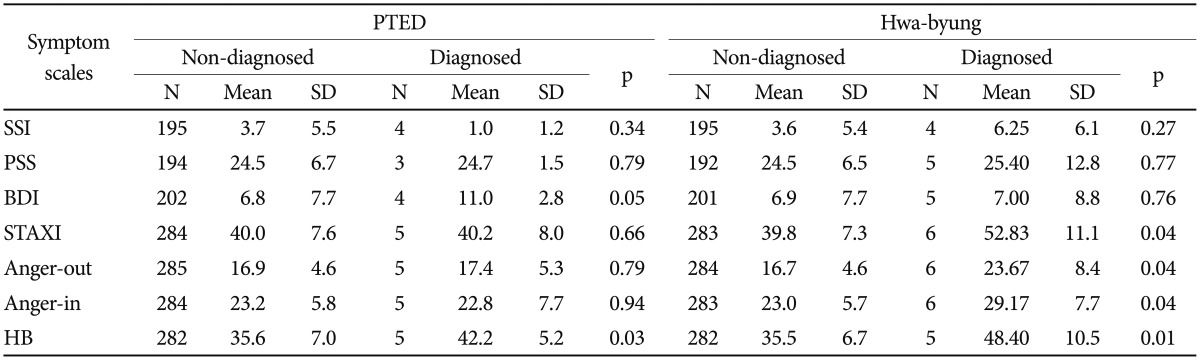
Psychiatric symptom scale scores were compared between individuals with and without PTED and those with and without Hwa-byung (Table 3). BDI scores were significantly higher among participants with PTED than those without. However, no statistically significant differences in STAXI scores were observed between the two groups. In contrast, STAXI scale scores were significantly higher among participants with Hwa-byung than those without. However, BDI scores were not significantly different between the two groups. Scores on the SSI and PSS were not significantly different between those with PTED and those without. Additionally, SSI and PSS scores did not differ significantly between those with Hwa-byung and those without. Finally, scores on the Hwa-byung scale were significantly greater among participants with PTED than those without.
DISCUSSION
The present study is the first to compare the prevalence and relationships among clinical variables related to PTED and Hwa-byung in a Korean cohort. Although the numbers of PTED and Hwa-byung diagnoses were small in the present study (owing mainly to the low prevalence rates in the general population), significant differences were observed between the PTED and Hwa-byung diagnostic groups for various clinical metrics.
Similarities and distinctions in PTED and Hwa-byung psychopathology
The present findings suggest some shared psychopathological components of PTED and Hwa-byung. For instance, individuals with PTED demonstrated higher Hwa-byung scale scores than those without PTED. Despite this commonality, some differences between PTED and Hwa-byung emerged, suggesting that they are separate disease entities. For instance, anger inhibition and expression was more strongly associated with Hwa-byung than with PTED; conversely, depression was more associated with PTED than with Hwa-byung. This suggests that PTED likely has a different pathogenesis than suppression or partial expression of anger as observed in Hwa-byung.
Further discrimination between the two disease states comes from results showing no co-occurrence of PTED and Hwa-byung in the present cohort. This was still the case when using more liberal disease criteria: i.e., only using criteria A (core symptoms) or B (accessory symptoms) provisions. Additionally, the number of individuals at higher risk for suicide and depression was significantly different between the Hwa-byung and non-Hwa-byung groups, but this was not the case in the PTED-diagnosed group relative to the non-PTED-diagnosed group.
Nevertheless, PTED and Hwa-byung have common psychopathological components and similar theoretical etiologies. As previously mentioned, embitterment, the core psychopathological symptom of PTED, is similar to the concept of ŌĆ£Haan/HahnŌĆØ in Hwa-byung.28 By definition, ŌĆ£HaanŌĆØ is a mixed feeling of missing someone, experiencing sorrow/regret/sadness and depression, and feelings of hatred and revenge. 171829 This is comparable to feelings associated with ŌĆ£embittermentŌĆØ in PTED. In addition, PTED and Hwa-byung are both reactive disorders related to daily stress.1320
However, PTED and Hwa-byung include several distinctions in terms of possible pathogenic mechanisms. First, acute stress is usually a critical factor in PTED while lifelong stress is more indicative of Hwa-byung. Second, PTED is attributed to the direct context of the adverse event(s).1314 In contrast, Hwa-byung onset is relatively insidious and not closely related to a specific event.17182030 Third, embitterment is assumed to be a direct reaction to stress.1314 However, the ŌĆ£HwaŌĆØ in Hwa-byung results from the forced suppression of anger toward a stressor, regardless of whether this suppression was successful or not.17182021303132 Finally, embitterment seems to focus more on present stressors, while Hwa-byung deals with unresolved and repressed emotional reactions to past stress.17182021303132 Thus, these differences between PTED and Hwa-byung may help explain discrepancies related to PTED and Hwa-byung diagnostics.
Prevalence of PTED and Hwa-byung
The prevalence of PTED in the general population was previously reported at approximately 2.5%.33 This rate is slightly higher than that reported in the present study (1.7%). The prevalence of Hwa-byung was also higher than PTED in South Korea. Such differences may be due to various forms of sampling or cultural differences. Reactions to stress may also differ depending on race, ethnicity, and culture. Furthermore, different social situations may influence the incidence of PTED and Hwa-byung.
Previously reported prevalence rates for Hwa-byung range from 4.2% to 13.3%.34353637 This is a much higher percentage than that observed in this study (2.1%). These differences may owe to different diagnostic criteria for Hwa-byung. Most past studies used self-labeling of Hwa-byung as the diagnostic criteria. 343536 Thus, the relatively low prevalence of Hwa-byung in this study may be explained by application of more structured and strict diagnostic criteria.
Depression and suicidality in Hwa-byung
In spite of exclusion of current psychiatric diagnosis and past suspected psychiatric disorders, many subjects showed depressive signs (12.1%) and suicidality (10.1%). This result can be explained by the high sensitivity of the measuring tools for depressive signs and suicidality used in this study. For screening tools, cut-off scores were decided by giving priority to sensitivity, and therefore a relatively high percentage of participants were found to be at risk for depression and suicide. In the standardization study for the Korean BDI, the cut-off value was determined the be the point at which 15.6% of subjects were classified as having depressive signs.25 This is consistent with our result. The same strategy was applied for the standardization of the Korean SSI. The estimated suicide ideation by the Korean SSI among Korean people ranges from 3.3% to 15.3% depending on the socioeconomic class of the participants.3839 In addition, South Korean society is highly suicidal because of the rapid transition from an agrarian to industrial society within a half-century and prolonged economic hardship since the exchange crisis in 1997.404142434445 In a study of the prevalence of past experience with suicide ideation the rate was found to be 12.5% in males and 23.1% in females in South Korea.46 Considering all the above, our results thus fall within a reasonable range.
Historical and sociocultural insights in PTED and Hwa-byung divergence
PTED was first described among unemployed immigrants from East and West Germany after the fall of the Berlin Wall.13 Prior to the reunification of Germany, society was more equitable across the country. However, after reunification, social and financial inequality among the population emerged as there was an influx of individuals migrating from West to East Germany.4748 South Korea has also experienced similar issues. Since the South Korean economic crisis of 1997, economic inequality has increased, and unemployment has worsened in recent years.49 However, the sociocultural underpinnings of PTED and Hwa-byung are a bit divergent. A single negative life event frequently associated with physical threat to life was related to PTED, whereas more chronic, life-long repetitive stressors mostly associated with psychological oppression were related to Hwa-byung.125051 In the case of Hwa-byung, unfairness related to social status and situations in which an individual tolerates irrationality and injustice for their present social survival and future plans is typical.5152 This divergence in the timeline between these two disease states and the stronger social and cultural underpinnings of Hwa-byung also helps to highlight their distinctions.
Hwa-byung is translated to either ŌĆ£fire-illnessŌĆØ or ŌĆ£anger-disease.ŌĆØ ŌĆ£HwaŌĆØ means both fire and anger.5253 Traditionally psychological stress is believed by Koreans to cause Hwa-byung.52 A large body of literature describes Hwa-byung occurring individuals who could not resist against or avoid long-lasting unfairness but rather had to endure it.30 Some researchers have suggested that Hwa-byung is a psychosomatic expression of suppressed psychological stress.1516 The oldest document describing Hwa-byung is found in ŌĆ£Sam-guk-sa-ki,ŌĆØ the history of three nations written by Bu-Shik Kim in the 10th century A.D.,54 which is the oldest history book in Korea. Although there are many literary descriptions of death by Hwa-byung,52 most Koreans who self-label as having Hwa-byung do not think they will die from Hwa-byung. However, death by Hwa-byung is suggestive of its somatizing characteristics. Patients with Hwa-byung typically complain of fever-sensations in the upper body, face, and head, a hard feeling on the chest, and/or lump in his or her throat.52 These manifestations have led to a theoretical model of Hwa-byung as a chronic psychosomatic disorders.16 Alternatively, Hwa-byung is considered a unique disorder resulting from prolonged exposure to unjust treatment and subsequent suppression of emotion;35 anger expression can be particularly difficult given the traditional Korean value, ŌĆ£Elders first, Social superiors first.ŌĆØ
While PTED focuses bitter ŌĆ£emotionŌĆØ itself toward unjust treatment, Hwa-byung focuses more on distorted expressions of emotion in situations in which patient cannot avoid or fight against chronic persecution and hide their anger and aggression from persecutors for their survival in society. This can be adaptive in order for patient's to maintain their social status in Korean society. Differences between Hwa-byung and some personality disorders can be explained in this context. With respect to Hwa-byung, anger-prone personality or impulsivity disorders emphasize individual sensitivity to stress.50 However, Hwa-byung may be a cultural adaptation toward inevitable and irresistible social frustration and humiliation. Although it is a socially acceptable way of dealing with stress, Hwa-byung causes an individual significant distress. Gradual transition from a patriarchal and vertical society to a democratic and horizontal society may alleviate personal distress caused by Hwa-byung.
Limitations
A few limitations of the present study should be noted. First, given the small number of PTED participants, some results should be interpreted with caution (and non-significant Fisher's exact test results should be acknowledged based on this limitation). However, the Mann-Whitney U tests results confirmed that PTED was not related to depression or suicidality. Second, random selection and age stratification were not applied during subject recruitment. However, the original sample size of 290 was large enough to be representative of the population. Demographic characteristics such as gender distribution, age distribution, and occupation distribution were similar across the survey population and representative of the entire Korean population.55 Third, it is an open question as to why PTED was not related to perceived stress, depression, and suicidality (which was the case for Hwa-byung) in the present study. Again, this could be due to a small sample size of PTED participants, age and gender composition, recruitment sources, or actual differences between these two disorders. Fourth, given the limited number of individuals in the diagnostic groups, direct comparisons between these groups were not tenable. Future studies should include a large sample of individuals diagnosed with PTED and Hwa-byung. Fifth, we excluded participants who reported that they were not currently diagnosed as having psychiatric disorders and have not been suspected as having psychiatric disorders. This may have underestimated the true prevalence of PTED and Hwa-byung because many patients with PTED and Hwa-byung show diverse psychiatric symptoms.1652 However, exclusion of those with a current psychiatric diagnosis prevented overdiagnosis of PTED and Hwa-byung, and may have reduced the possibility of mistaking symptoms of other psychiatric disorders, such as mood disorders, for symptoms of Hwa-byung and PTED. Finally, the cross sectional study design used limits insights into possible diagnostic changes across both disorders. Thus, a longitudinal design would be useful to confirm diagnostic stability across these disorders.
Conclusions
The present study suggests that PTED and Hwa-byung have different clinical features. The study also suggests that embitterment is not merely a feeling of inner anger as is often associated with Hwa-byung. Hwa-byung was related more to the suppression or partial expression of anger, while PTED was more associated with depression. Finally, the results indicate that PTED and Hwa-byung is not an overlapping diagnosis.