INTRODUCTION
Early-onset bipolar disorders are characterised by a severe and repeated course accompanied by mixed episodes, psychosis, and suicidal thoughts and behaviours.12 The initial presentation often appears as a depressive episode, which leads to the misdiagnosis of unipolar depression; children who were diagnosed with unipolar depression prior to puberty have high risks of bipolar spectrum disorders,3 more than half of unipolar depressed patients are estimated to change diagnosis within the next 20 years.4
There are prominent irritabilities without elated mood in the bipolar depression of adolescents, and irritability is also a common symptom in both mania and depression phase.56 A mixed episode is often prominent in children and adolescent bipolar depression, which has been related to an increased possibility of suicidal attempts.7 Moreover, depressive or mixed episodes are more likely to recur compared with a manic episode in children and adolescents.89 A study which reported the clinical characteristics of Korean early-onset Bipolar disorder patients, reported more psychotics symptoms and comorbid psychiatric disorder compared to bipolar disorder patients who had onset after 19 years of age, however there was no difference in suicidal attempt rate, rapid cycling pattern, and report of familial loading of bipolar illness.10 Due to lack of appropriate rating tools and confusion with natural tumultuousness of adolescence, there is difficulty in the diagnosis of bipolar depression in adolescents. The delayed diagnosis of bipolar depression as unipolar depression results in the under-treatment of depressive symptoms in young individuals, which undermines development in environmental and neurobiological aspects.11 Therefore, the proper and early diagnosis and treatment are crucial for adolescents to avoid long-term adverse outcomes.
Bipolar depression is phenotypically different from unipolar depression and rating scales originally designed for unipolar depression scales do not fully capture the documented psycho- pathological differences.12 Depression rating scales, such as the 17-item Hamilton Depression Rating Scale (HAM-D),13 the Inventory of Depression Symptomatology (IDS)14 and the Montgomery-Asperg Depression Rating Scale (MADRS),15 fail to assess key elements of the severity or treatment response in bipolar disorder.16 Berk et al.17 previously developed the Bipolar Depression Rating Scale (BDRS), which is a specialised tool for measuring bipolar depression that includes atypical features and mixed states. BDRS arguably better captures symptoms in bipolar depression especially depressive mixed states than traditional unipolar depression rating scales.16 Validation of BDRS in adolescents is particularly timely in the context of recent changes in DSM-5 which have expanded the definition of mixed episode to include subthreshold manic symptoms.18
Moreover, there are limited tools specialised for depression in children and adolescents, including the Children's Depression Inventory (CDI), Children's Depression Rating Scale (CDRS) and the Centre for Epidemiological Studies Depression Scale for Children (CES-DC). However, these tools also evaluate patients based on unipolar depression. Furthermore, there are studies that have failed to show significant differences between the depressed and non-depressed groups using these conventional tools based on unipolar depression,1920 which have raised questions as to the validity of these tools in the assessment of depressive symptoms in adolescents with depression. However, the BDRS was developed and standardized for adults, not for adolescents. In the present study, we explored the feasibility and psychometric properties of the Korean version of the BDRS in adolescent patients with Early-onset bipolar disorders.
METHODS
Participants
Forty depressed patients, aged 13-18 years, with a diagnosis of bipolar disorder were enrolled in this study and the comparison group included 13 euthymic bipolar disorder patients. Of the 40 depressed patients, 5 patients transitioned to the euthymic state after treatment; these patients were included in both the depressed and euthymic groups, which resulted in 40 depressive patients and 18 euthymic patients. The subjects were recruited from the outpatient clinics and inpatient wards of one national centre for child and adolescent psychiatry. To minimize the inter-rater differences in patient assessment, one board-certified psychiatrist conducted the structured interviews using the K-SADS-PL, and conducted the HAM-D, the MADRS, the Young Mania Rating Scale (YMRS), the Modified Overt Aggression Scale (MOAS) and the Korean version of BDRS. The HAM-D and the MADRS assessed depression symptoms, the YMRS assessed mania symptoms, and MOAS rated aggression. Treating psychiatrists carefully reassessed the diagnosis and the mood symptom assessment afterwards to correlate with clinical profile of the patients.
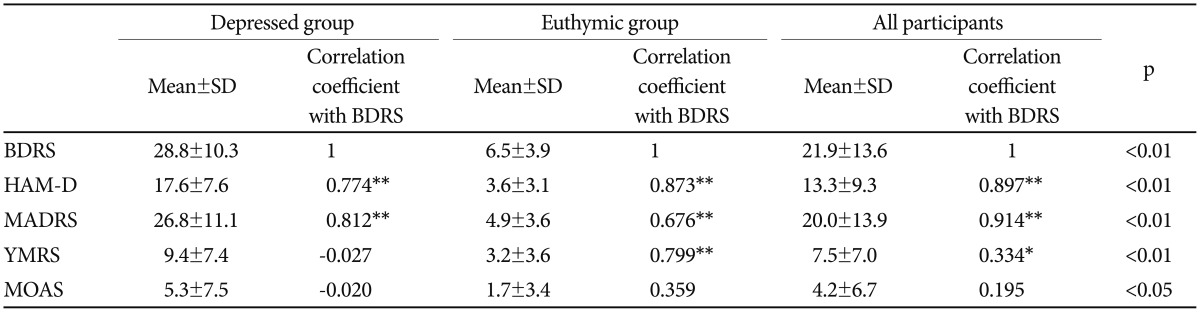
The patients were diagnosed using Kiddie Schedule for Affective Disorders and Schizophrenia Present and Lifetime (K-SADS-PL), which is a semi-structured diagnostic interview, considered as a gold standard for diagnosis of affective disorder in children and adolescents. Mean score on the HAM-D of depressed and euthymic group was 17.6±7.6 and 3.6±3.1, MADRS was 26.8±11.1 and 4.9±3.6, respectively. Patients with severely impaired cognitive function, substance abuse, unstable medical problem, and current history of organic brain disease (e.g., seizure) were excluded from participating in the study. All research procedures were approved by the Institutional Review Board (IRB) of Seoul National Hospital, and all participants provided informed consent for the study. All study procedures were in accordance with the latest version of the Helsinki declaration.
Instruments
Bipolar Depression Rating Scale
The standardization of the Korean version of the BDRS (K-BDRS) was performed by Chang et al.21 for adults patients, which suggests that the K-BDRS has an advantage in evaluating bipolar depression. The BDRS is a semi-structured observation tool used to evaluate bipolar depression. It is particularly sensitive to the evaluation of atypical and mixed symptoms. Composed of 20 items, each item is evaluated on a 4-point scale (0, 1, 2, and 3 represent no, mild, moderate, and severe symptoms, respectively), and the total score range is 0-60. If the obtained score is higher, then the severity of depression can be considered higher. Items 1 to 15 evaluate the core symptoms of depression. The sleep and appetite categories (items 2 and 3) are divided into increase and decrease characteristics, thereby evaluating hypersomnia and overeating, which are common in bipolar depression. Items 16 to 20 (i.e., irritability, lability, increased motor drive, increased speech, and agitation) evaluate mixed symptoms, which are common features in bipolar disorder.17
Hamilton Depression Rating Scale
The 17 item HAM-D13 was originally developed to assess the effectiveness of antidepressant treatment and is often used in studies of adolescents, and previous study has shown that the test-retest reliability at 1 week was good (r=0.9) in a study of a small number of adolescents.22 Internal consistency was also good in a sample of depressed and nondepressed high school students (α=0.91).23 Each item on the questionnaire is scored on a 3 or 5 point scale, depending on the item with higher scores indicating more depression. Generally, a score of 0-6 is evaluated as normal, 7-17 is mild depression, 18-24 is moderate depression and higher than 24 is severe depression.24 Korean Version of HAM-D was standardized with good internal consistency (Cronbach's alpha coefficient=0.76) and inter-rater reliability.25
Montgomery-Asperg Depression Rating Scale
The MADRS15 is 10 item scale, which assessapparent sadness, reported sadness, inner tension, reduced sleep, reduced appetite, concentration difficulties, lassitude, inability to feel, pessimistic thoughts, suicidal thoughts.26 Items are scored on a 6-point scale. Scores range from 0 to 60, with higher scores indicating more depression. Previous studies showed that when the adolescents with major depression were compared to adults with major depression rated by MADRS, depressions among adolescents and adults had similar symptomatology.27 A score of 10 or below indicates normal and a score greater than 35 indicates severe depression.2829 Korean version of MADRS was standardized with good internal consistency (Cronbach's alpha coefficient=0.79).30
Young Mania Rating Scale
The YMRS31 is an 11-item scale, which assesses the intensity of manic symptoms based on a clinical interview with the patient and takes into account the subjective comments of the patients and the clinician's own observation. Out of 11 items, 4 items are scored on 8 point score, 7 items are scored on 4 point score, with higher scores indicate more mania symptom. Korean version of YMRS was standardized with acceptable internal consistency (Cronbach's alpha coefficient=0.73).32 Previous studies have been conducted to validate its use with children and adolescents, which have also shown satisfactory psychometric properties.333435
Statistical analysis
Statistical analysis was performed with SPSS 19.0 for windows (SPSS Inc., Chicago, IL, USA). Frequency analysis and descriptive statistics were used in the demographic analysis and partial correlation coefficient; data were controlled for age and gender in the correlation coefficient between the total score and items. Cronbach's alpha coefficient and the item to total score correlation were used to confirm the internal consistency of the BDRS. Pearson correlations between the BDRS, HAM-D, MADRS, YMRS and MOAS were examined to verify scale validity. To investigate internal structure of BDRS, principal component analysis with a varimax rotation and hierarchical cluster analysis was conducted. All analysis were conducted in depressed group. Chi-square and fisher's exact test were performed to compare demographic characteristics between depressed and euthymic groups. In order evaluate discriminative validity, ANCOVA adjusted for demographic characteristics were conducted to compare depressive and euthymic groups.
RESULTS
Participant characteristics
In the depressed group, there were 23 males and 17 females, with a mean age of 15.7±1.6 years (Table 1). The mean onset age was 12.3±3.0 years. In terms of diagnoses, there were 25 bipolar I disorder (62.5%) patients, 10 bipolar II disorder (25.0%) patients, and 5 bipolar disorder NOS (12.5%) patients. Categorised by treatment patterns, there were 9 outpatients (22.5%), 29 closed ward patients (72.5%), and 2 day-hospital patients (5.0%). There were 10 males and 8 females in the euthymic group, with an average age of 14.9±1.6 years; the average onset age was 12.2±2.4 years. In the euthymic comparison group, there were 12 bipolar I disorder (66.7%) patients, 5 bipolar II disorder (27.8%) patients, and 1 bipolar disorder NOS (5.6%) patients. There were 7 outpatients (38.9%), 9 closed ward inpatients (50.0%), and 2 day hospital patients (11.1%). When depressed and euthymic groups were compared, there were no significant differences in age, gender, onset age, and diagnoses.
Internal consistency of BDRS in depressed group
Cronbach's alpha coefficient was 0.843 in depressed group, which indicates a high internal consistency of the BDRS. Cronbach's alpha values were re-calculated for the BDRS scale by systematically removing each of the items for the depressed group (0.83-0.86). For item to total BDRS score correlation, all items except items 18 (increased motor activity) and 19 (increased speech) showed high correlation in depressed group. The results show that internal consistency of the scale is stable and that no single item disproportionately disturbed the homogeneity of the scale.
Discriminative validity and inter-correlation among instruments
The average BDRS score of the depressed group was 28.8±10.3, while the HAM-D average was 17.6±7.6 and the MADRS average was 26.8±11.1. The average scores of the YMRS and MOAS were 9.4±7.4 and 5.3±7.5, respectively. For all of the scales, the depressed group showed significantly higher score compared to the euthymic groups (Table 2). There was positive correlation coefficient was between the BDRS and HAM-D and also between BDRS and MADRS (r=0.774, p<0.01 for HAM-D; r=0.812, p<0.01 for MADRS) in depressed and euthymic group. There were no significant correlations between the BDRS total score and the YMRS or MOAS (Table 2). For item to total MOAS score correlation, two items ‘irritability’ and ‘lability’ showed high correlation (Table 3).
Endorsement rates of the items on the BDRS in depressed group
The item ‘depressed mood’ showed the highest endorsement, followed by ‘worthlessness’, ‘reduced activity’, ‘reduced social engagement’, and ‘helplessness’ (Table 4). ‘Increased motor drive’ (7.5%) and ‘increased speech’ (10%) was least endorsed followed by ‘agitation’ (27.5%) and psychotic symptom (35%). About half of the patients endorsed ‘irritability’ (47.5%) and ‘lability’ (55%), and there were nine depressed patients (21%) who had atypical symptoms of ‘hypersomnia’, whereas ten (23%) patients exhibited ‘hyperphagia’.
Internal structure of BDRS indepressed group
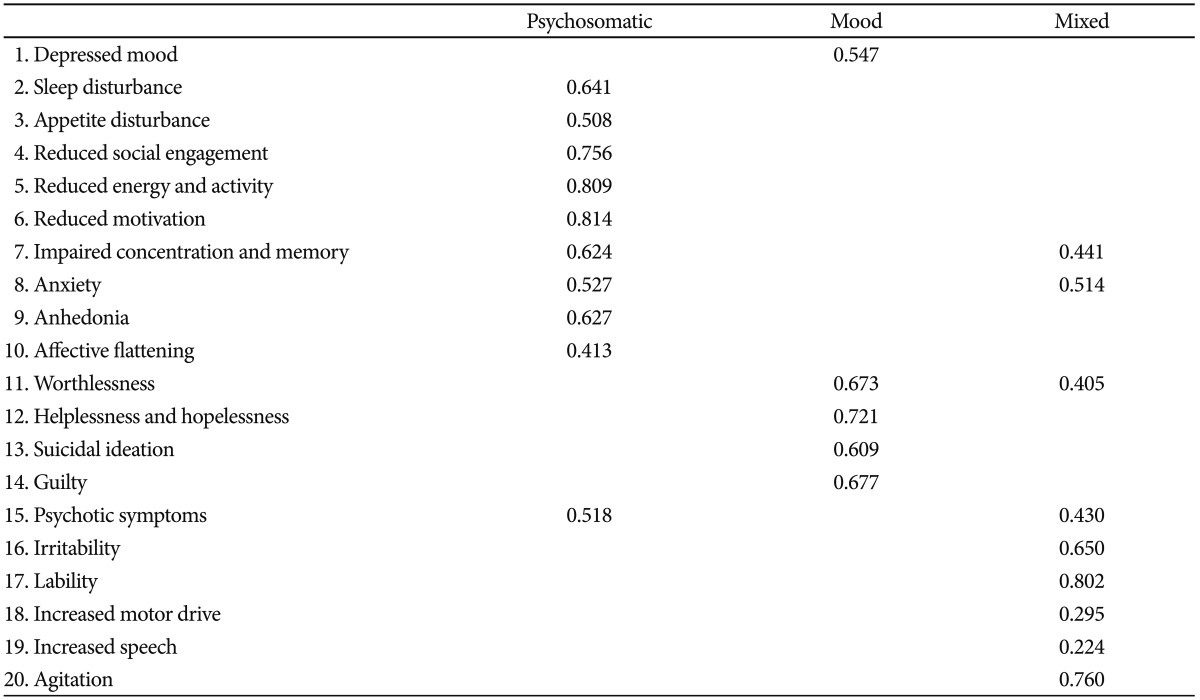
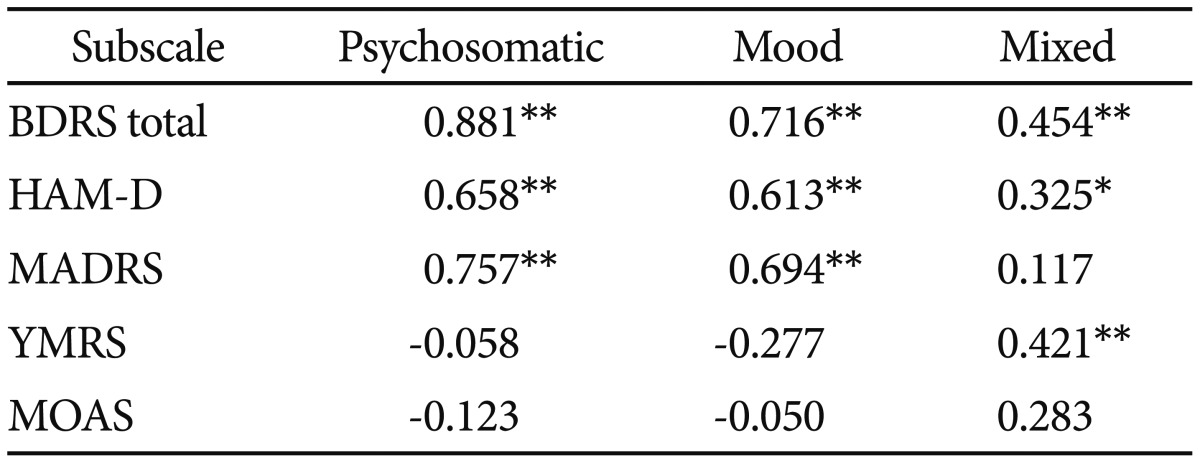
The factor structure of the BDRS was explored using principal component analysis with a varimax rotation. The Kaiser criterion (eigenvalue greater than 1) was applied to determine the number of significant factors. Three factors were extracted from the factor analysis of 20 items in the BDRS with varimax rotation, ‘psychosomatic’ depression, ‘mood’, and ‘mixed’; the items in each factor are reported in Table 5. When analysing correlations between scales based on the three factors and the BDRS, HAM-D, MADRS, YMRS, and MOAS totals, ‘psychosomatic’ and ‘mood’ factor showed strong positive correlations with the BDRS, HAM-D, and MADRS total scores. While the ‘mixed’ factor showed correlations with the BDRS, HAM-D, and YMRS total scores (Table 6).
Hierarchical cluster analysis was also performed on 20 items of BDRS (Figure 1). These were divided into three main clusters like principal component analysis, but elements of clusters were somewhat different the clusters of factor analysis. Irritability and lability were included in the mood cluster and agitation was moved from the mixed cluster to the psychosomatic cluster. Only increased motor drive and increased speech remained inthemixed cluster.
DISCUSSION
This study explored the feasibility and psychometric properties of the Korean version of the BDRS in adolescents with Early-onset bipolar disorders. In this research, the BDRS showed good internal consistency, high reliability and validity similar to the results from previous studies performed with adult subjects with bipolar depression,17213839 which indicates that the BDRS is also a useful tool for evaluating adolescents with Early-onset bipolar depression. Cronbach's alpha of the BDRS was 0.843, which demonstrated very high internal consistency, and was significantly correlated with other depression rating tools, such as the HAM-D and MADRS. Moreover, when the mean total score was compared between the depressed and the euthymic groups diagnosed using K-SADS-PL, the BDRS total scores of the depressed group was significantly higher compared with the euthymic group, which demonstrate concurrent validity indicating that the BDRS is a valid tool for the assessment of depression. Furthermore, in item score to total score correlations, all items except ‘increased motor drive’ and ‘increased speech’ showed significant correlations. The items ‘increased motor drive’ and ‘increased speech’ are items that belong in the mixed subscales, and previous studies have also shown that the correlations of these two items with the BDRS total score were low.1738
In the factor analysis, there were three factors consistent with the original standardization study of the BDRS,17 however, there were differences in the components. In the original standardization of the BDRS by Berk et al., the factors were divided into psychological depression (anhedonia, worthlessness, helplessness, and guilt), somatic depression (reduced concentration and activity and disrupted sleep and appetite), and mixed factor (psychotic symptoms, lability, and increased motor drive and speech). However, in this study, sleep and appetite disturbances, reduced social engagement, reduced activity, reduced motivation, impaired concentration, anxiety, anhedonia, affective flattening and psychotic symptoms were considered ‘psychosomatic’ depression, and the symptoms related to ‘psychological’ depression, such as depressed mood, worthlessness, helplessness, guilty and suicide ideation composed another factor classified as ‘mood.’ Mixed factor was composed of irritability, lability, increased motor, increased speech and agitation. But in cluster analysis, only increased motor drive and speech were included in mixed cluster. In Chang et al.,21 cluster analysis showed two cluster structure, the first cluster was depressive symptom cluster which consisted of 12 items and second cluster was mixed symptom cluster which consisted of 8 items including increased motor drive and speech, lability, irritability, agitation, suicidal ideation, appetite disturbance, and psychotic symptoms.
The differences in factor components compared with previous studies that have explored the factors of the BDRS may reflect the differences between adult and adolescent symptomatology in bipolar depression or the differences between the phenomenological manifestations between adult-onset bipolar disorder and early-onset bipolar depression. The results of the present study suggest that irritability, lability and agitation are more general depressive feature of adolescent's bipolar depression. It also correspond with the changes in DSM-5 criteria of bipolar disorder depressive episode with mixed features, where irritability was excluded from mixed symptoms because it appears frequently in depression.4041 The ‘psychosomatic’ depression and ‘mood’ factors had strong correlations with the other depression rating scales, while ‘mixed’ factors showed correlations with the HAM-D and the YMRS. The MOAS showed weak positive correlations with all of the factors but items ‘irritability’ and ‘lability’ showed correlation with total MOAS score, suggesting that ‘irritability’ and ‘lability’ is associated with aggression in early-onset bipolar depression.
In Korean adults with bipolar depression, the mean HAM-D score was 16.2 (SD=7.0) and the mean MADRS score was 24.5 (SD=8.8),21 which is similar to the mean HAM-D (17.6±7.6) and the mean MADRS (26.8±11.1) of depressed adolescents in this study. However, the score of YMRS was 5.0 (SD=6.8) for adult Korean bipolar depression patients,21 whereas the mean YMRS score was slightly higher for adolescents at 9.4 (SD=6.8) in this study. The mean total BDRS score was 23.3 (SD=7.8) for adult Korean bipolar depression patient,21 whereas for adolescents the mean total BDRS score was higher at 28.8 (SD=10.3). These results again suggest that more mixed feature is present in adolescent bipolar depression compared to adult bipolar depression, but direct comparison between adult and adolescent bipolar depression patients is required in the future.
The items that showed the highest endorsement with the BDRS total scores were ‘depressed mood’ and ‘worthlessness’ followed by ‘reduced activity,’ ‘reduced social engagement’ and ‘helplessness.’ One of the unique features of the BDRS is that sleep and appetite can be discriminated into an increase and decrease of sleep or appetite. In this research, there were 9 depressed patients (21%) who had ‘hypersomnia,’ whereas 10 patients (23%) exhibited ‘hyperphagia’. Moreover, nearly half the patients exhibited moderate to severe ‘irritability’ or ‘lability,’ demonstrating that irritability and lability is indeed frequent in adolescent bipolar depression. Also, ‘agitation,’ which showed a weak correlation with the total score in adult depression,173839 was also reported as moderate to severe in one quarter of the patients. These findings are very interesting because it suggest that atypical and mixed symptoms are frequent in adolescent bipolar depression, along with the core symptoms that have been reported in adult onset bipolar depression.42
In this study, some patients were rated as mildly depressive on HAM-D and MADRS although clinically they showed moderate to severe depression, indicating that it is difficult to properly evaluate adolescents' bipolar depression by conventional tools based on unipolar depression. So, we can infer that the BDRS has strength over conventional depression rating scales in the assessment of adolescent bipolar depression, which is characterized by prominent irritabilities without elated mood56 and mixed episodes.7 Moreover, impulsivity and delinquent behaviour is also common and serious issue in adolescent's depression.4344 As irritability and lability are associated with these aggressive behaviors, focusing on these symptoms will be helpful in evaluation of behavioral issues in adolescents with bipolar depression.
The present study has several limitations. First, all of participants were Korean limiting the generalizability of the findings. Second, because of the relative difficulty of diagnosing bipolar depression at early age, the sample size is relatively small. Because considerable number of participants were diagnosed with bipolar II disorder or bipolar disorder NOS without distinct manic episodes, we cannot rule out the possibility that some of the patients may be diagnosed with other psychiatric conditions when they grow up. However, we should take into account that most bipolar patients have yet to experience manic episodes in adolescents.4546 Also there are limited diagnostic tools currently available for adolescent bipolar disorder. We performed clinical evaluation and structured diagnostic interviews in order to increase the reliability and validity of bipolar diagnosis in adolescents with bipolar depression. However, it is necessary to verify our findings in larger cohorts for future studies. Third, limited availability of age appropriate depression rating scale in Korean language has made the use of child specific depression rating scales impossible, therefore we used Korean version of HAM-D and MADRS. It is important that future efforts should be made to standardize Korean version of children and adolescent specific depression rating scale. Fourth, the subjects did not include unipolar depression patients as a comparison group. Therefore direct comparison between symptom structures of unipolar depression and bipolar patient group were not possible.
In conclusion, Korean version of BDRS exhibited good internal validity and significant correlations with the HAM-D and MADRS scores in adolescents with Early-onset bipolar disorders. All items on the BDRS were significantly correlated with the BDRS total scores except for increased motor activity and increased speech. Importantly, in comparisons of the BDRS scores between the depressed and euthymic groups diagnosed using K-SADS-PL, the depressed group scored higher compared with the euthymic group. The BDRS was useful in evaluating the mixed and atypical symptoms, as well as depressive symptoms of early-onset bipolar depression. In this explorative study of the BDRS for adolescents with Early-onset bipolar disorders, we suggest that the BDRS may be a feasible and reliable tool for the assessment of bipolar depression in adolescents with early-onset bipolar disorders. Given the worldwide burden of bipolar disorder across the lifespan and the controversies about early presentations of this disorder in non-US populations, validating diagnostic assessments for use clinically and in research settings is important. This exploration of BDRS in adolescents with bipolar depression will also enable clinical studies for assessment of the adolescent patients with unipolar depression in comparison with bipolar depression so that we may identify the differences between unipolar and bipolar depression in the future.