INTRODUCTION
Driving is the ŌĆśultimateŌĆÖ instrumental activity of daily living (IADL) [1] as it requires integration of high-level cognitive functions, motor functions, and perception [2,3]. For the elderly, ceasing to drive can interfere with their independent living and decrease their autonomy [4]. It may also decrease access to social activities, household activities (e.g. shopping), and medical services, thus increasing feelings of isolation and depression [5,6]. Previous studies have pointed out that ageing itself does not necessarily impair driving or increase the risk of car accidents [7,8]. However, older people have a high prevalence of cognitive impairment and dementia that may increase the risk of unsafe driving [9]. Motor dysfunction in ParkinsonŌĆÖs disease and AlzheimerŌĆÖs disease can predict driving performance [10,11]. Since driving abilities of the elderly are linked to safety, it is important to identify factors affecting driving abilities of the elderly population.
White matter hyperintensity (WMH) is described as area showing increased signal on T2-weighted magnetic resonance image (MRI) including fluid attenuated inversion recovery (FLAIR) image. It generally shows the degree of subcortical ischemic change [12]. Previous studies have shown that WMH is associated with cognitive dysfunctions such as global cognitive performance, executive function, processing speed [13], and motor dysfunction such as gait dysfunction [14]. Cognitive and motor dysfunctions combined can negatively affect driving performance in the older population. However, only a few studies have reported the association between the degree of WMH and driving capacities in the elderly.
Therefore, the objective of this study was to investigate the association between WMH and driving cessation in the elderly using a nationwide multicenter hospital-based prospective cohort. Whether the degree of subcortical ischemic changes on MRI could predict the risk of driving cessation in the elderly with or without motor and cognitive dysfunctions was determined in this study.
METHODS
Participants
This study was conducted as a part of the Clinical Research for Dementia of South Korea (CREDOS) study, a nationwide multicenter hospital-based prospective cohort study aimed to understand characteristics of Korean patients with dementia. The CREDOS study was conducted from November 2005 to April 2013. It had developed common protocols, including Clinical Evaluation Form and Caregiver Questionnaire Form. It recruited patients with subjective memory impairment, mild cognitive impairment, mild cognitive impairment of subcortical vascular type, and AlzheimerŌĆÖs disease. All patients underwent comprehensive interviews including complete medical history, physical examinations, neurological examinations, neuropsychological assessment, and MRI scans. Brain MRI scans included transaxial T2- and T1-weighted scans and fluid-attenuated inversion recovery (FLAIR) slices. CREDOS neuroimaging visual rating scale was developed by the CREDOS study central committee based on scales of Fazekas [15] and Scheltens [16] with modifications. It was described as ŌĆ£Assessment of White Matter Hyperintensities.ŌĆØ A more detailed description of the CREDOS study such as inclusion and exclusion criteria is available elsewhere [17]. The CREDOS study was approved by the Institutional Review Boards of all participating hospitals (AJIRB-MED-SUR-12_027). Written informed consent was obtained from patients and their caregivers after informing them about details of the study. We retrospectively analyzed 540 subjects with data available about driving status at baseline who were followed up at least once after the first visit (mean┬▒SD follow-up duration: 2.13┬▒1.54 years). Follow-up data of 370 MRI scans were available.
Clinical evaluation and calculation of composite score for motor dysfunction
Clinical Evaluation Form included the follwoing: 1) history of cognitive decline from the caregiver, 2) Mini-Mental State Examination (MMSE) [18], 3) CDR Sum of Boxes score (CDR-SOB) [19], and 4) neurological examination. The Caregiver Questionnaire Form included the following: 1) basic demographic data about the patient and the caregiver, 2) lifestyle including driving status classified as ŌĆ£Now drivingŌĆØ, ŌĆ£Not drivingŌĆØ, or ŌĆ£Driving cessation (driven before, not driving now)ŌĆØ, 3) Barthel activity of daily living (ADL) index [20], and 4) Seoul Instrumental ADL (S-IADL) [21]. In this study, a total of 540 patients with ŌĆ£Now drivingŌĆØ or ŌĆ£Driving cessation (driven before, not driving now)ŌĆØ status at baseline driving evaluation were selected.
All patients underwent neurological examinations, including motor function evaluations such as rigidity, bradykinesia, hemiplegia, ataxia, and Parkinsonian features in relation to gait function. Based on these results, motor dysfunction was scored 0 when there were no abnormalities in any feature. Otherwise, it was scored 1.
Neuropsychological tests and calculation of composite scores for cognition
All subjects underwent Seoul Neuropsychological Screening Battery (SNSB), a standardized neuropsychological test [22]. This battery contained tests for attention, language, visuoconstructive function, memory, and frontal/executive function. Scorable tests included Digit Span Backward (DSB), Korean version of Boston Naming Test (K-BNT) [23], Rey-Osterrieth Complex Figure Test (RCFT), Seoul Verbal Learning Test (SVLT), and Color Word Stroop Test (CWST). Age-, sex-, and education-specific norms for each test based on 447 normal subjects were available [22]. From these tests, composition score for cognition in relation to driving ability was calculated by summing Z-scores of CWST-color reading, DSB, RCFT-copy, and RCFT-delayed recall reflecting executive function, attention, and visual perception, respectively.
Assessment of WMH
Three neurologists trained in rating ischemic white matter changes who were blinded to clinical and functional data rated white matter changes on T 2 axial and/or FLAIR images. CREDOS WMH rating scales were developed by the CREDOS study central committee based on FazekasŌĆÖ scale [15] with modifications. The longest diameter of white matter changes around lateral ventricles (capping or banding on periventricular areas) or in the white matter (especially the centrum semiovale) was evaluated separately. Periventricular white matter changes were rated as P1 (<5 mm), P2 (Ōēź5 mm, <10 mm), or P3 (Ōēź10 mm). Deep white matter changes were rated as D1 (<10 mm), D2 (Ōēź10 mm, <25 mm), or D3 (Ōēź25 mm). These results were combined to give a final ischemia score of mild, moderate, or severe. Combinations of D1 with P1 (D1P1) and D1 with P2 (D1P2) were classified as ŌĆśmildŌĆÖ. Combinations of D2P1, D3P1, D2P2, D3P2, D1P3, and D2P3 were classified as ŌĆśmoderateŌĆÖ while combinations of D3 and P3 (D3P3) were classified as ŌĆśsevereŌĆÖ.
Statistical analyses
We compared patients with three different degrees of white matter changes on MRI. A Žć2 test was performed to examine trends in categorical data. Analysis of variance (ANOVA) was performed for continuous variables to compare groupsŌĆÖ scores for demographics and driving status. To evaluate the relative effect of WMH on driving with or without mediation of cognition and motor function, a structured equation model (SEM) was used. We used generalized estimating equation (GEE) to estimate longitudinal effects of WMH on change in driving status. All statistical analyses were performed using SPSS version 22.0 for demographics, AMOS 21.0 for SEM (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. IBM Corp., Armonk, NY, USA), and GEE package of R version 3.1.2 for GEE [A language and environment for statistical computing (Version 3.1.2). Vienna, Austria: R Foundation for Statistical Computing].
RESULTS
Demographics and clinical data according to the degree of WMH
We analyzed demographic and clinical characteristics according to the degree of WMH. At baseline, 389, 116, and 35 patients were classified as ŌĆśmildŌĆÖ, ŌĆśmoderateŌĆÖ, and ŌĆśsevereŌĆÖ, respectively. According to the degree of WMH, there were statistically differences in age, sex, driving cessation, and motor dysfunction score. DSB, Rey Osterrieth Complex Figure (ROCF)-delayed recall, and CWST-color reading on SNSB also showed statistical differences among the three groups (Table 1).
Association of WMH with driving cessation, cognition, and motor dysfunction
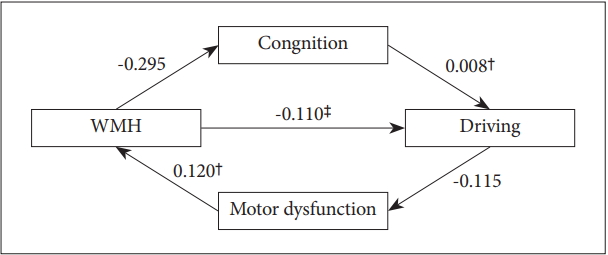
The model (Table 2, Figure 1) depicted both direct and the indirect relationships of WMH with driving cessation, cognition dysfunction, and motor dysfunction. Direct path from WMH to driving status was statistically significant (╬▓=-0.110, p<0.001). WMH was significantly associated with motor dysfunction score (╬▓=0.120, p<0.001) and cognition was predictive of driving cessation (╬▓=0.008, p=0.01). However, WMH to cognition (╬▓=-0.295, p=0.486) or motor dysfunction score to driving status (╬▓=-0.115, p=0.093) showed no significance. All model fit indices were good (Žć2=12.173, df=1, p<0.001, Comparative Fit Index=0.834, Goodness of Fit Index=0.989, Adjusted Goodness of Fit Index=0.890, Root Mean Square Residual=0.078).
WMH and progression from ŌĆ£now drivingŌĆØ status to ŌĆ£driving cessationŌĆØ status
We examined individual differences in the rate of change from ŌĆ£Now drivingŌĆØ status to ŌĆ£Driving cessationŌĆØ status using generalized estimating equation models after controlling for age, sex, and education. To examine the relationship between the degree of WMH and the rate of decline in ŌĆ£Now drivingŌĆØ status, we added a baseline and repeatedly measured degrees of WMH to determine their interaction with time (unadjusted model). In this model, there was a strong association between the rate of change in driving status from ŌĆ£Now drivingŌĆØ to ŌĆ£Driving cessationŌĆØ and repeatedly measured degrees of WMH from baseline. Age, sex, or education did not affect the association between the degree of WMH and change in driving status. It remained significant (╬▓=-0.542, p<0.001).
We repeated the model and added terms of several covariates such as composite scores for cognition (Cognition) and composite scores for motor dysfunction (Motor Dysfunction) to determine its effect on the relationship between rate of change in driving status from ŌĆ£Now drivingŌĆØ to ŌĆ£Driving cessationŌĆØ and repeatedly measured degrees of WMH from baseline. The addition of terms for Cognitive or Motor Dysfunction did not change the association between the degree of WMH and change in driving status. It remained significant (╬▓=-0.508, p<0.001) (Table 3).
DISCUSSION
This study aimed to examine the association between the degree of WMH and driving cessation in a large cohort study using carefully clinical interviews, neurologic examinations, neuropsychological tests, and MRI scans. Findings of this study showed that the degree of subcortical ischemic changes might be one of predictive factors for driving ability in the elderly with or without mediation of cognitive or motor dysfunction in both cross-sectional and longitudinal aspects.
Due to difficulty in testing driving performance on a road test, the gold standard test for driving competence [24], a few studies have explored predictors of driving cessation such as the proxy report of IADLs or cognitive battery [25]. Cognitive functions, motor functions, and perception are known to be critical for safe driving [2,3]. In the cognitive domain, previous studies have shown that visual attention, executive function, and visual perception are among the most important factors affecting driving ability [26-33]. A composite score reflecting test performances across multiple cognitive domains is known to be a predictor of driving safety for persons with AlzheimerŌĆÖs disease [10]. It has been reported that driving performance starts to decline in early disease stage of AlzheimerŌĆÖs disease [10,34]. Disease progression and severity have been found to be predictors for driving deterioration [34-36]. In motor functions, the Functional Reach test used for detecting balance impairment has been found to be a probable predictor for driving competence [37,38]. Pegboard test for motor coordination and motor speed and the Get-Up-and-Go task used as part of a global assessment of an individualŌĆÖs fall risk [39] might also be predictive of driving performance [11]. Results of the present study are consistent with previous studies about the association of driving ability with cognitive and motor functions in cross-sectional and longitudinal aspects.
Few previous studies have investigated relationships of driving cessation with both cognitive and motor dysfunctions through an integrated approach. The degree of WMH is known to reflect both cognitive and motor function. WMH reflects disruption of longitudinal tracts located in periventricular and subcortical white matter regions in the brain that link motor function and executive function. It could interfere with bidirectional transfer of information between key motor and cognitive cortical regions [40-42]. Previous studies have reported that WMH is associated with motor decline such as decreased gait speed and increased gait number [43-48]. These findings are consistent with results of the present study showing that the degree of WMH can significantly affect motor function which could affect gait function. Meanwhile, WMH could be regarded as a potentially useful intermediate marker to identify cognitive impairment [13]. Previous studies have suggested that WMH is associated with global cognitive performance [13] and specific cognitive deficits such as impaired recall, slowing processing speed, deficient executive planning [49,50], and ADL impairment [51-53]. In our study, there was no significant relationship between WMH and cognition in SEM. Such difference in result might be due to demographic confounding factors and various neurodegenerative factors such as amyloid burden, cerebrovascular disease, and brain atrophy which could not be evaluated in this study [54].
Interestingly, this study showed that the direct path from WMH to driving status was statistically significant in SEM. In this study, GEE models demonstrated that over time, the more severe the change in the degree of WMH, the more rapid the deterioration in driving performance. This association remained significant after adjusting for age, sex, education, cognition score, and motor dysfunction score known to be crucial for driving competence. Collectively, in both cross-sectional and longitudinal aspects, the association between the degree of WMH and driving is direct and significant. Considering that a surrogate imaging marker has the potential to predict the natural course of the disease with possibility to correlate with relevant clinical features in both cross-sectional and longitudinal studies [55], WMH might be an independent predictive factor for driving cessation in the elderly with or without mediation of cognitive or motor dysfunction.
This study had several limitations. First, other reasons to quit driving such as economic problems were not taken into consideration. Second, the actual decline of driving ability or the risk of an accident could not be determined because driving status was only evaluated by using caregiver questionnaires. Third, MRI finding was classified only by WMH without considering cortical atrophy, lacuna, or others. Fourth, data on driving-sensitive cognitive or motor functions were limited. Further studies are needed to evaluate cognition and motor functions through specific tests focusing more on driving such as actual driving.
Despite these limitations, this study was a well-defined cohort study to report the degree of WMH and its association with driving cessation. Qualified and systematic tests evaluating cognitive functions and MRI scan were used and results were significant even after adjusting for covariates. In conclusion, subcortical ischemic changes on MRI may be an independent predictive factor for driving cessation. It could indirectly reflect both motor and cognitive functions.