INTRODUCTION
Since the outbreak of coronavirus disease-2019 (COVID-19) in China in December 2019, the pandemic has spread to various countries across the world, including Korea. As a result, medical service needs have increased, and doctors have become overworked. Additionally, mental health problems, such as depression, anxiety, insomnia, post-traumatic stress, perceived stress, mental pain, and burnout, continue to emerge [1-3]. In fact, even before the outbreak of COVID-19, mental health problems were becoming increasingly prevalent among doctors owing to their high job demands.
Burnout is the physiological, emotional, and mental exhaustion resulting from long-term involvements in emotionally burdensome environments [4]. Burnout affects an individual’s body and psychology, and it negatively affects their ability to carry out their professional duties optimally [5]. The World Health Organization developed the International Classification of Diseases 11th revision in which burnout was included as a job-related phenomenon in “factors affecting health status or use of health services.” [6] It is imperative to measure the effect of burnout among doctors because burnout can affect doctors’ mental health as well as the quality of treatment they provide. In a meta-analysis of studies conducted in 45 countries from 1991 to 2018, 67% of the doctors surveyed experienced burnout [4]. Doctors who experience burnout tend to be authoritative or cold when dealing with patients, thereby making it difficult to ensure that patients feel comfortable. Such doctors also make it difficult to determine appropriate treatment methods, and they do not communicate effectively with their fellow medical personnel and patients [7]. In addition, according to a survey of US doctors conducted in 2014, 54% reported experiencing more than one burnout, and 10.5% reported making significant medical mistakes over the past three months [8,9].
The most frequently used measure for evaluating burnout is the Maslach Burnout Inventory (MBI) which requires a licensing fee to be used. In the MBI, a high level of job burnout is defined as a high score in emotional burnout and depersonalization as well as a low score in personal achievement [10]. When the MBI was first developed, the scope of application was limited to human service occupations, such as nursing, teaching, and social work-related occupations [11]. In this case, the Maslach Burnout Inventory-Human Services Survey (MBI-HSS) [12] was used. However, recently, the concept of job burnout was expanded to include more comprehensive occupations, thereby resulting in the development of the Maslach Burnout Inventory-General Survey (MBI-GS) [13]. Afterwards, the Maslach Burnout Inventory-Student Survey (MBI-SS) was also developed. The MBI-SS, which is a modified version of the MBI-GS, was designed to evaluate burnout among students [14].
Various studies on mechanisms related to the improvement of doctors’ mental health have been conducted using burnout measurement tools. Such mechanisms include organizational strategies, financial return on investments, and evidence-based strategies [15-17]. Therefore, it is essential to regularly check for the presence or absence of burnout among doctors to improve their mental health. However, currently, there is an overall lack of studies on burnout among doctors in Korea. Additionally, the use of multiple questions makes it difficult to measure burnout among doctors with extreme fatigue and high workloads [8,9,18]. To solve this problem, Pomeroy et al. [19] argued that brevity and ease would be of significant help to the effective evaluation and follow-up of burnout among doctors because most respondents are not willing to spend a lot of time responding to questions in survey tables. In fact, many studies rely on a single question scale to evaluate burnout among doctors [20-22].
Self-diagnoses of burnout are based on emotional exhaustion [23], thereby making the relationship between the MBI subscale and a single question-based burnout assessment based on one’s definition particularly relevant. Rohland et al. [24] and Hansen and Girgis [20] validated the single-item burnout measure (SIBM) compared to the MBI-HSS in physicians. Both concluded that the SIBM could be effectively used as an alternative to the Maslach Burnout Inventory-Emotional Exhaustion (MBI-EE) for screening burnout.
The objective of this study is to validate a Korean version of the SIBM, which was developed to rapidly measure the level of burnout among doctors.
METHODS
Participants and procedure
To conduct online surveys, survey URLs were distributed to all public health doctors (n=1,621) actually practicing in the period from July 2021 to August 2021 in South Korea, and the participants volunteered. The subjects were South Koreans who graduated from medical school, general practitioners, interns, or specialists who completed residency training and worked as public health doctors at public health centers, public hospitals, national health research institutes, and other consignment organizations instead of military service. A total of 324 copies (20%) were collected from July 22 to August 5, 2021, and 294 people’s data were analyzed, excluding 24 duplicate surveys and six cases determined to be extreme values. Of these, 269 (91.5%) had experience of being dispatched to work related to COVID-19. This study was approved by the clinical research ethics committee of Eulji University College of Medicine and Hospital (IRB No. 2021-04-013).
Measurements
A demographic questionnaire was used to collect relevant information, such as gender, age, marital status, and employment information, regarding the participant group. Data provided by public health doctors regarding burnout were obtained using the SIBM and MBI-GS. The scales used to verify the convergence validity were the Patient Health Questionnaire-9 (PHQ-9), Generalized Anxiety Disorder-7 (GAD-7) screening tool, Perceived Stress Scale (PSS), and MBI-GS. Additionally, the Vaccination Attitudes Examination (VAX) scale was used to verify the discriminant validity.
SIBM
The SIBM was first introduced in a survey of HMO physicians by Schmoldt et al. [25], whereby respondents were asked to classify their level of burnout using their definition of burnout [25-27] and has been used in several studies regarding physician burnout in US. Rohland et al. [24] compared the SIBM to the MBI-HSS in Texas medical school graduates. In Australia, Hansen and Girgis [20] also compared the two versions among Australian oncology medical professionals, including doctors and nurses. The simple correlation (r) between the SIBM and MBI-EE was 0.64 and 0.68 in the two studies, respectively, and the R2 obtained by analysis of variance (ANOVA) was evaluated as 0.5 in both studies, suggesting that it can be effectively used as an alternative to MBI.
The responses were scored using a 5-category ordinal scale, and the items were dichotomized into burnout or not through the following classifications: a score of ≤2 was categorized as having no symptoms of burnout, and a score of ≥3 (definitely burning out) was categorized as having one or more symptoms [25,28].
Two Korean psychiatrists who were fluent in English translated the SIBM into Korean, and the Korean version was translated back into English by English and Korean bilingual. After repeating translation and reverse translation, the final translation was selected in consideration of the sociocultural characteristics of Korea. The questions presented in the translated version of the SIBM presented in Supplementary Table 1 (in the online-only Data Supplement).
MBI-GS
The MBI-GS is a self-report test designed for evaluating burnout. It comprises three subscales: exhaustion, cynicism, and professional efficacy. The MBI was included in its entirety, and the subscales were scored as directed by the MBI Manual, third edition [10]. The Korean version of the MBI-GS was translated by Shin [29], and its validity was verified. Authorization to use the MBI-GS was purchased from Mind Garden (Menlo Park, CA, USA). It comprises five questions on exhaustion, four on cynicism, and six on professional efficacy, making 15 questions in total. Owing to the work characteristics of public health doctors, the MBI-GS was used to measure the stress of the work itself because most of the samples collected did not involve patient interviews. The internal consistency coefficients of the subscales were α=0.90 for exhaustion, α=0.86 for cynicism, and α=0.85 for professional efficacy [29].
PHQ-9
The PHQ-9 is a self-report test designed for screening depression and evaluating the severity of depression. The Korean version of the PHQ-9 was adapted and validated by Han et al. [30]. A self-report test was also developed by Spitzer et al. [31] using the diagnostic criteria for major depressive disorders presented in the Diagnostic and Statistical Manual of Mental Disorders, fourth edition. It comprises nine items, and it is a test for determining how often such problems have been experienced over the past two weeks. The responses are evaluated using a 4-point scale of “no,” “for a few days,” “more than a week,” and “almost every day,” and the range of scores comprises 0 to 27 points. In this study, the sensitivity and specificity levels in the domestic PHQ-9 standardization study were reviewed, and nine points were used as reference points and as cutoff values for whether depression was screened among healthy group participants [32,33]. Cronbach’s α of the Korean version of the PHQ-9 was 0.85-0.95 and the optimal cutoff point for major depression was 9 in the PHQ-9 [32,33]. The internal consistency coefficients were α=0.91 in our study.
GAD-7
To screen generalized anxiety disorders and assess the severity of symptoms, GAD-7, which was developed by Spitzer et al. [34], was used. In Korea, Seo and Park [35] translated the GAD-7 screening tool and used it to conduct a study on migraine patients, and the internal consistency was 0.915. The GAD-7 screening tool was designed for use among primary care patients. The GAD-7 screening tool comprises a self-report questionnaire that identifies symptoms of generalized anxiety disorder. The participants are asked whether they were bothered by anxiety-related problems over the past two weeks by answering seven items on a 4-point scale. Ahn et al. [36] suggested a cutoff of the Korean version of GAD-7 with 8 points, and Cronbach’s α in their study was 0.93.
PSS
The PSS was developed by Cohen and colleagues [37,38], and it was revised in 1988. This scale proves reliability and validity using self-reported tests for evaluating experiences of perceived stress over the past one month using a 5-point Likert scale. In the 10-item PSS, questions 1, 2, 3, 6, 9, and 10 are scored as positive questions, whereas questions 4, 5, 7, and 8 are scored as negative questions. The total score ranges from 0 to 40 and the higher the total score, the more severe the perceived stress. Lee et al. [39] validated the Korean version of the PSS, and reported Cronbach’s α as 0.819 and test-retest reliability coefficient as 0.66.
VAX scale
The VAX scale is a 12-item scale (including four subscales) used to assess anti-vaccination attitudes. This scale was developed by Martin and Petrie [40]. The VAX Korean version, which was translated and reverse-translated by a certified translation company and reviewed and confirmed by two Korean medical doctors, was used, but there is no validation study yet. The results of the factor analysis on this scale of our study subjects, like the scale developers’ results [40], include four factors: trust/mistrust of vaccine benefits (item 1-3), worries over unforeseen future effects (item 4-6), concerns about commercial profiteering (item 7-9), and preference for natural immunity (item 10-12). The internal consistency coefficient (α) for Korean version of VAX was 0.90. And internal consistency for the subscales (Cronbach’s α) was 0.83 (trust of vaccine benefits), 0.79 (worries over unforeseen future effects), 0.91 (concerns about commercial profiteering), and 0.79 (preference for natural immunity), respectively, showing good-to-excellent internal consistency.
Statistical analysis
Demographic results were identified through frequency analysis, and Pearson correlation analysis was used to obtain the convergent and discriminant values. The relationship between each of the MBI subscales and the question in the SIBM was assessed using paired ANOVA and simple Pearson correlation coefficients. The ANOVA analyses compared each of the MBI subscales using the categorical responses to the question in the SIBM. Simple correlation coefficients were also calculated for each of the MBI subscales and the self-defined burnout question. In addition, to understand the relationship between depression and anxiety according to burnout, the prevalence was calculated using cross-analysis. For statistical analysis, we used SPSS version 21.0 (Data Solution Inc., Seoul, Korea).
RESULTS
Demographic results
The average age of the participants was 29.59 (standard deviation [SD]=2.39) years, and the number of interns, intern graduates, and specialists was 166 (56.5%), 69 (23.5%), and 59 (20.1%), respectively. Other demographic variables are listed in Table 1. The prevalence of burnout through the SIBM was 133 (45.2%) out of 294 participants.
The prevalence of depression through the PHQ-9 was 82 (27.9%) out of 294 participants, and the prevalence of anxiety through the GAD-7 screening tool was 44 (15.0%). The mean score of stress measured using the PSS was 17.23 (SD=5.79), the vaccine attitude score measured using the VAX scale was 33.02 (SD=7.23), and the burnout score measured using the MBI-GS was 44.44 (SD=14.83) (Table 2).
Comparison of the SIBM to the MBI and other scales
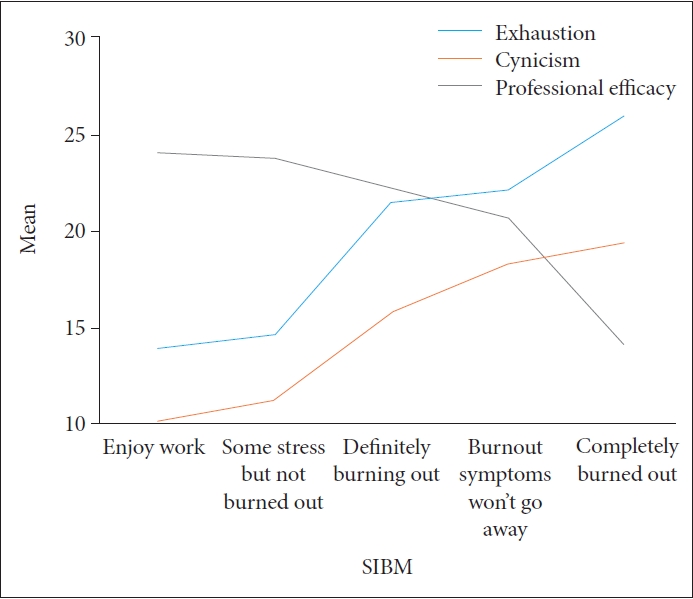
As a result of one-way ANOVA, the total score of the MBI-GS and the mean and SD for each answer of the SIBM were 36.04 (SD=14.18), 38.12 (SD=13.23), 51.13 (SD=11.47), 55.80 (SD=14.33), 67.29 (SD=10.72), and R2=0.27 (p<0.01). The R2 of “emotional exhaustion”, a subscale of MBI-GS, was 0.27 (p<0.05), the same as that of the total score of MBI-GS. The R2 of the other two subscales, “cynicism” and “professional efficacy,” were 0.20 (p<0.05) and 0.06 (p<0.05), respectively. So “professional efficacy,” was less associated with the single-item measure. Pearson’s correlation analysis also showed a positive correlation between the total score (r=0.50, p<0.01), “emotional exhaustion” subscale (r=0.43. p<0.01), “cynicism” subscale (r=0.48, p<0.01) and “professional efficacy” subscale (r=0.22, p<0.01) (Table 3).
Figure 1 shows the relationship between the SIBM and the subscales of MBI-GS using ANOVA. More responses to SIBM’s “completely burned out” increased levels of “exhaustion” and “cynicism,” while decreasing “professional efficacy” (Figure 1).
As a result of additional convergent validity verification with related scales, the correlation coefficient between the SIBM and the PHQ-9, GAD-7, PSS, and MBI-GS was a positive correlation (p<0.01), and thus, convergent validity was verified. In addition as a result of verifying the discriminant validity, the correlation coefficient between the SIBM and the VAX scale was not significant. Therefore, discriminant validity was verified (Table 2).
Prevalence of depression and anxiety with and without burnout
Depression and anxiety were evaluated through the cutoff values of the PHQ-9 (≥9) and the GAD-7 (>7), and then the prevalence of each was confirmed according to the presence or absence of burnout. Among those with and without burnout, depression was 68 (51.1%) vs. 14 (8.7%), and anxiety was 39 (29.3%) vs. 5 (3.1%), respectively, showing significant differences (p<0.01) (Figure 2).
DISCUSSION
As a result of analyzing data obtained from 294 public health doctors in Korea, the convergence validity and discriminant validity were verified. By comparing the SIBM and the MBI-GS using ANOVA, the performance of the Korean version of the SIBM was verified with regards to the total score and subfactors of the MBI-GS: burnout, cynicism, and professional efficacy. Although the MBI-HSS was used in Rohland et al. [24], these three components of MBI-GS almost coincide in meaning with the three dimensions of the MBI-HSS. Exhaustion is a concept that is consistent with the emotional exhaustion of the MBI-HSS, and cynicism refers to feeling a sense of distance from an individual’s job as well as experiencing a negative attitude toward the overall job. Compared to the second subcomponent of the MBI-HSS, depersonalization, the difference is that the object of negative attitude or distance has changed from the person or individual to the work itself, i.e., the job. Professional efficacy is characterized by a low sense of self-efficacy, the lack of a sense of accomplishment, the lack of performance, and helplessness [29]. In Rohland et al. [24] the score was R2=0.498 for the SIBM and its extension and 0.27 for this study. However, the score for professional efficiency was similar, and in the case of cynicism, it was 0.144 in Rohland et al. [24] and 0.20 in this study. Therefore, it can be concluded that the results of Rohland et al. [24] and those of our study are consistent.
Meanwhile, the prevalence of burnout among the participants of this survey was approximately 45.2%. This is similar to the prevalence rate of 40% to 60%, which was found in a number of studies conducted on foreign doctors [4,41,42]. In this study, the prevalence of depression in subjects with burnout was 51.1%, which was similar to the results of Shechter et al. [43] and Lai et al. [1] for doctors. In addition, the prevalence of anxiety in people with burnout in this study was 29.3%, which was similar to the 20%-30% presented in other studies conducted by doctors [2,29]. This is consistent with the findings of previous studies showing the relationship between depressive symptoms and burnout and showing a direct proportional relationship between the degree of depression and the severity of burnout [44]. Similarly, Ding et al. [45] found that emotional exhaustion and cynicism, which are subfactors of the MBI-GS, were positively associated with anxiety symptoms, whereas professional efficacy was negatively associated with anxiety symptoms.
Although this study succeeded in deriving remarkable results, there were some limitations. First, this study involves a random sample of only public health doctors in Korea. Therefore, there exist limitations associated with generalization. As a result, in future studies, it is necessary to examine whether our approach is applicable to all groups of doctors using various methods, such as radio sampling and stratified sampling. Second, in this study, because only male public health doctors were surveyed, it may be difficult to apply the overall approach to all genders. Therefore, in future studies, it seems that enhanced objective evaluation will be possible if data are collected from doctors of both genders. Third, this study did not correct the familywise error that could be caused by the multicorrelation test. Future research needs to consider these aspects.
Despite these limitations, the SIBM, which comprises a single question, is significantly useful. Currently, the problem of burnout among doctors continues to persist as the COVID-19 pandemic progresses [46,47]. Additionally, burnout continues to affect doctors’ mental health, the quality of medical services, and patient satisfaction. Therefore, appropriate intervention strategies are required at the group and national levels [7,15-17]. In this situation, the fact that the SIBM comprises a single question and can be implemented and scored rapidly without the need to calculate the score will be helpful for ensuring continuous follow-up. This is because the relative brevity of the SIBM compared to the 15-item MBI might help to enhance participation among physicians who have traditionally low response rates. In addition, the SIBM is significantly advantageous in that it does not carry any licensing fees, and it is easy to interpret because the response explicitly indicates the presence or absence of burnout. Therefore, it is considered useful to use a Korean version of the SIBM that can be simply evaluated to enhance continuous follow-up observations and response rates to emotional exhaustion. This version of the SIBM can be a useful tool for various settings with limits on time and resources. Therefore, it is expected that this version of the SIBM could be widely used to detect burnout in many occupational settings.
Conclusion
In this study, we validated an evaluation tool that can measure burnout using a single question. The validity of convergence and discrimination was identified by comparing correlations with other scales, and the SIBM was evaluated as a measurement tool with appropriate validity through the comparison of the mean and SD of the MBI-GS subscales. Compared to the existing methods for evaluating burnout, the SIBM can be evaluated rapidly without the need for calculating the score because it uses a single question. This attribute makes it useful in various environments with limited time and resources. Therefore, this evaluation tool is expected to make it easy for doctors to prevent and treat various symptoms, such as depression and anxiety, associated with burnout because it allows for continuous follow-up when evaluating burnout.