INTRODUCTION
Schizophrenia is a severe psychiatric disorder characterized by positive symptoms, negative symptoms, and cognitive deficits. It affects approximately 1% of the world’s population and ranks as one of the top 10 global causes of disability [1]. Cognitive impairment is one of the core features of schizophrenia, involving a series of impaired neurocognitive functions. This impairment is critically associated with patients’ recovery of social functions and long-term outcomes, while pharmaceutical therapy and psychosocial interventions have limited effects on its improvement [2,3]. Therefore, it is crucial to have a deep understanding of the related risk factors of cognitive impairment in schizophrenia.
Studies in the general population have indicated that several metabolic factors are associated with cognitive impairment and dementia, including diabetes or increased fasting plasma glucose concentrations, abdominal obesity, hypertension, and dyslipidemia [4,5]. A cluster of these metabolic risk factors has been termed metabolic syndrome (MetS) [6,7]. In schizophrenic patients, the prevalences of metabolic risk factors are significantly higher than in the general population [8]. The high prevalence may be due to the pathology of the disease and the side effects of antipsychotic treatment [8]. The relationship between metabolic risk factors and neurocognitive deficits has also been investigated in schizophrenia, and available studies suggest that the occurrence of metabolic risk factors and MetS can worsen existing cognitive impairment in schizophrenia [9-12]. A meta-analysis published in 2021, including 10,174 schizophrenic patients, indicated that the presence of metabolic risk factors and MetS are significantly associated with cognitive deficits in patients [13]. These findings suggest that improving metabolic risk factors and MetS may help manage cognitive impairment in schizophrenia.
Notably, in the general population, researchers have found that the association between metabolic risk factors and cognitive function is affected by sex [14-16]. For example, Huo et al. [16] found that specific risk factors (diabetes and dyslipidemia) have stronger associations with cognitive decline for women than men. Schuur et al. [15] reported that MetS was associated with poorer executive function only in women. Sex differences have been found in many aspects of schizophrenia, such as disease incidence, age of onset, clinical symptoms, response to treatment, long-term outcome, and social functions [2,17]. Male patients have an earlier age of onset, more severe negative symptoms, and worse long-term disease outcomes [17,18]. Studies also suggest sex differences in brain morphology and cognitive function in schizophrenia. For instance, neuroanatomical studies have found that the morphological abnormalities of the brain are more evident in male patients than in female patients [17]. Studies also found that male patients experience more cognitive impairments than female patients, especially in verbal learning and memory tasks [19,20]. Although several studies have explored the relationship between metabolic risk factors and cognitive function in schizophrenia, few studies have investigated the impact of sex on their association.
Taken together, these findings prompt us to raise the question of whether sex affects the association between metabolic risk factors and cognitive function in schizophrenia patients. If so, it could help us to tailor the treatment of metabolic risk factors by sex stratification in patients, resulting in better improvement of their cognitive deficits. Therefore, the primary purpose of this study is to investigate the association of metabolic risk factors with cognitive deficits in schizophrenic patients based on sex. The secondary purpose is to investigate the impact of sex on cognitive deficits and the rate of metabolic risk factors in schizophrenic patients.
METHODS
Subjects
All participants recruited were Han Chinese and aged between 18 and 65 years. Patients were recruited from Shanghai Mental Health Center, Shanghai Civil Affairs First Mental Health Center, Cixi Mental Health Center, Quzhou Third People’s Hospital, and Huzhou Third People’s Hospital between January 2017 and January 2020. All patients who met the diagnosis of schizophrenia were included, and the diagnosis was made by experienced psychiatrists according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. Patients with any other major Axis I disorder, such as mental disorders due to a general medical condition, delirium, dementia, amnestic and other cognitive disorders, mood disorders, acute stress disorder, and schizoaffective disorders, were excluded. We have excluded the patients with comorbidity of depressive disorders. Because depressive disorder is highly correlated to cognitive function and more common in women, which can affect the interpretation of results. Healthy controls were recruited from the local community through advertisements. Both patients and healthy controls were interviewed by trained raters using the Mini-International Neuropsychiatric Interview to confirm the clinical diagnosis of schizophrenia or to screen whether the controls have any major Axis I disorder diagnosis. Healthy controls with a personal or family history of psychiatric disorders were excluded. Furthermore, participants with cerebral vascular disease, central nervous system diseases, severe physical diseases, substance abuse/dependence, pregnancy, or lactation were also excluded. Finally, 358 schizophrenic patients (244 males and 114 females) and 231 healthy controls (111 males and 120 females) were included in the statistical analysis.
The protocol was reviewed and approved by the Ethics Committee at Shanghai Mental Health Center (IRB No. 2019-35R). Written informed consent was obtained from all subjects before the study.
Clinical assessment and cognitive evaluation
Sociodemographic information and clinical characteristics, such as sex, age, education, height, weight, age of onset, duration of illness, antipsychotics use, and other medications, were collected using the self-designed questionnaire. Clinical symptoms were assessed using the Positive and Negative Syndrome Scale (PANSS) [21]. The inter-rater correlation coefficient for assessments was greater than 0.8.
The cognitive function of participants was assessed using the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS, Form A) [22], which consists of 12 subtests that are used to calculate five age-adjusted index scores and a total score. The test indices include Immediate Memory (comprised of List Learning and Story Memory tasks), Visuospatial/Constructional (comprised of Figure Copy and Line Orientation tasks), Language (comprised of Picture Naming and Semantic Fluency tasks), Attention (comprised of Digit Span and Coding tasks), and Delayed Memory (comprised of List Recall, Story Recall, Figure Recall, and List Recognition tasks).
Assessment of metabolic indexes
Body mass index (BMI) (kg/m2) was calculated by dividing weight (kg) by height (m) squared. A trained research nurse measured blood pressure and waist circumference. After an overnight fast, blood samples were collected between 7:00 and 9:00 AM on an empty stomach. Serum fasting blood glucose (FBS), triglycerides (TG), and high-density lipoprotein cholesterol (HDLC) levels were measured by technicians who were blind to the diagnostic status of subjects.
Criteria of metabolic risk factors
Metabolic risk factors were defined using the following criteria: 1) Abdominal obesity: a waist circumference ≥90 cm in Chinese men and ≥80 cm in Chinese women; 2) Dyslipidemia: TG ≥1.7 mmol/L, or use of any lipid-lowering drugs; 3) Dyslipidemia: HDLC <1.03 mmol/L in men and <1.29 mmol/L in women, or use of any lipid-lowering drugs; 4) Hypertension: systolic blood pressure (SBP) ≥130 mm Hg or diastolic BP (DBP) ≥85 mm Hg, or treatment for hypertension; and 5) Hyperglycemia: FBS ≥5.6 mmol/L, or use of any antidiabetic medications. Subjects satisfying any three of the above correspond with the definition of MetS.
Statistical analysis
Kolmogorov-Smirnov one-sample test was used to detect the normal distribution of variables. Student’s t-test and analysis of variance (ANOVA) were performed on continuous variables, chi-square test or Fisher’s exact test for categorical variables. A 2×2 ANOVA (diagnosis×sex) was performed to assess the main effects of diagnosis and sex, as well as their interaction on demographic variables. Using education and BMI as the covariates, 2×2 analysis of covariance (ANCOVA) (diagnosis×sex) were used to explore whether the sex difference in cognitive scores would vary between patients and controls, taking the five RBANS subset score and total score as the dependent variable, respectively, and diagnosis and sex as fixed factors. After adjusting for duration of illness and BMI as covariates, logistic regression was used to compare the sex difference in the rate of metabolic risk factors and MetS in patients.
The multiple linear regression analyses investigate the association of metabolic risk factors and MetS with cognitive performances separately in male and female patients. The RBANS total and subscale scores served as the dependent variables. As covariates, age, education level, PANSS negative score, and BMI were included in the multiple linear regression analyses. Multiple comparison correction was applied using a false discovery rate. The results were presented with corrections for multiple testing. All statistical analyses were performed in IBM SPSS (version 26.0; IBM Corp., Armonk, NY, USA). Statistical significance was defined as p<0.05 (two-tailed test).
RESULTS
Sex differences in demographic, clinical variables, and cognitive performance in patients and healthy controls
As shown in Table 1, 358 schizophrenic patients (244 males and 114 females) and 231 healthy controls (111 males and 120 females) were recruited. The duration of illness for patients was 190.55±144.88 months. No significant difference in age was found between the two groups (schizophrenia: 40.59± 13.10 years vs. controls: 39.40±13.50 years). There were significant main effects of diagnosis with regard to education and BMI (all p<0.05). Schizophrenic patients had lower education levels and higher levels of BMI than controls. There were no significant differences in age and education levels between males and females in patients or the controls (all p> 0.05). Table 2 showed that male patients had a longer duration of illness than females (208.19±146.23 months vs. 152.90± 135.07 months, t=3.26, p=0.001) (Table 2). No significant sex difference was found in the age of onset, antipsychotic treatment, and PANSS scores (all p>0.05) (Table 2).
After controlling for education and BMI, 2×2 ANCOVA showed significant main effects of diagnosis in RBANS total and 5-subscale scores, which were all significantly lower in schizophrenic patients compared to healthy controls (all p< 0.001) (Table 1). There were no significant interactive effects of diagnosis×sex on any score were found (all p>0.05) (Table 1). Further subgroup analyses showed no significant sex differences in any cognitive score no matter in patients or controls (all p>0.05).
Sex differences in metabolic index levels and rates of metabolic risk factors
As shown in Table 2, male patients had significantly higher levels of waist circumference, SBP, DBP, and lower levels of HDLC (all p<0.05). Taking duration of illness and BMI as covariates, the logistic regression showed that the rate of abdominal obesity was lower in male patients (odds ratio [OR]=0.35, 95% confidence interval [CI]=0.17-0.71; χ2=8.36, df=1, p=0.004) (Table 3) than that in female patients. The rate of hypertension in male patients was significantly higher than that in female patients (OR=2.53, 95% CI=1.43-4.48; χ2=10.20, df=1, p=0.001) (Table 3). There was no significant sex difference in the rates of hyperglycemia, dyslipidemia, and MetS among patients (all p>0.05).
Sex difference in the association of metabolic risk factors with cognitive performances in patients
As shown in Table 4, we found dyslipidemia was negatively associated with the total score (β=-0.195, p=0.017), subscales of language (β=-0.199, p=0.017, pFDR=0.043), attention (β=-0.191, p=0.028, pFDR=0.047), and delayed memory (β=-0.243, p=0.007, pFDR=0.035) in female patients. In male patients, hyperglycemia was significantly associated with the subscales of immediate memory (β=-0.204, p=0.002, pFDR=0.010). Abdominal obesity, hypertension, and MetS were not significantly associated with cognitive function in male or female patients.
Considering the correlations among these metabolic risk factors, we further performed the multivariate regression analysis. After controlling for the other three metabolic risk factors, hyperglycemia was still significantly correlated with immediate memory score in male patients with schizophrenia (β=-0.230, p=0.001) (Supplementary Table 1 in the online-only Data Supplement). Similarly, dyslipidemia was still significantly associated with the total cognitive score (β=-0.286, p=0.002), and subscales of language (β=-0.196, p=0.029), attention (β=-0.223, p=0.024), and delayed memory (β=-0.328, p=0.002) in female patients with schizophrenia (Supplementary Table 2 in the online-only Data Supplement).
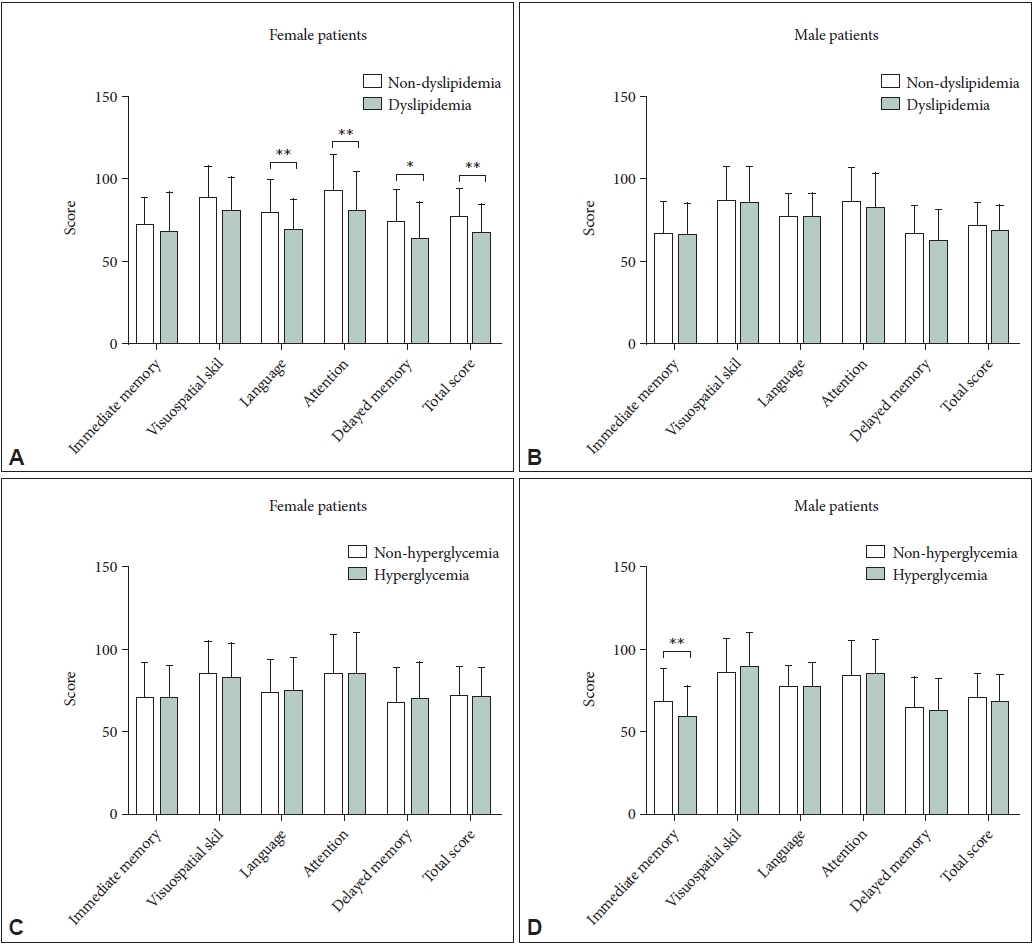
After controlling for the duration of illness, 2×2 ANCOVA showed significant interactive effects of dyslipidemia×sex on total scores (F=4.51, p=0.034) and aspects of cognitive performance including language (F=7.52, p=0.006) and attention (F=4.09, p=0.044) in patients with schizophrenia. Furthermore, we compared the cognitive scores of the non-dyslipidemia group with the dyslipidemia group by sex. In female patients, patients with dyslipidemia had significantly lower RBANS total scores (t=2.76, p=0.007) and aspects of cognitive performance including language (t=2.70, p=0.008), attention (t=2.79, p=0.006), and delayed memory (t=2.26, p=0.026) (Figure 1). However, no significant difference was found in RBANS total scores and all aspects of cognitive performance between the dyslipidemia and non-dyslipidemia group in male patients (all p>0.05) (Figure 1). In addition, after controlling for the duration of illness, the interactive effect of hyperglycemia×sex on immediate memory was not statistically significant (F=2.66, p=0.104). Further subgroup analyses showed that the hyperglycemia group had lower immediate memory than the non-hyperglycemia group in male schizophrenic patients (t=3.39, p=0.001) (Figure 1).
Within the healthy group, no significant associations of metabolic risk factors with cognitive scores were found for either men (all p>0.05) (Supplementary Table 3 in the online-only Data Supplement) or women (all p>0.05) (Supplementary Table 4 in the online-only Data Supplement).
DISCUSSION
Our study revealed significant sex differences in the rate of abdominal obesity and hypertension. Specifically, we revealed a higher rate of abdominal obesity and a lower rate of hypertension among female patients compared to their male counterparts. Additionally, our findings suggest that sex may influence the relationship between metabolic disorders and cognitive function in schizophrenia. Specifically, the analysis revealed that hyperglycemia emerged as a major risk factor for cognitive impairment in male patients, whereas dyslipidemia emerged as the primary risk factor for cognitive dysfunction in female patients.
Our study supports previous findings that patients with schizophrenia exhibit significant cognitive impairment compared to healthy controls [23]. However, we did not observe any sex differences in the degree of cognitive impairment in patients, which is consistent with the results reported by Zanelli et al. [24] and Kao et al. [25] Actually, although many studies relying on neuropsychological battery [17,26-29] and neuroimaging [30-32] have examined the impact of sex on cognitive function in schizophrenia, the conclusion remains controversial. These inconsistencies may be attributed to differences in symptomatology, medication status, illness onset, and illness duration between studies. In addition, the effect of sex on neurocognitive function in schizophrenic patients may be affected by the differences in sex hormones levels of participants when recruited, such as the different menstrual cycle stage of the woman and the reproductive stage of both sexes.
We found female patients had a higher rate of abdominal obesity than male patients. The higher rate of abdominal obesity in female patients was also reported in the previous studies [33,34]. Sex difference in the rate of abdominal obesity may attribute to the differences in the pharmacokinetics and pharmacodynamics of antipsychotic drugs between males and females [33]. Females are reported to have slower rates of drug absorption, metabolism, and excretion and have higher dopamine sensitivity than males [35,36], which may make female patients more vulnerable to weight gain and abdominal obesity, for the reason that antipsychotics lead to increased appetite and food intake through antagonistic effect on several neurotransmitter systems [37]. On the other hand, sex difference in the rate of hypertension in patients may attribute to the differences in blood pressure regulatory mechanisms between males and females [38,39], including the differences in the adrenergic receptors, reninangiotensin system (RAS), oxidative stress, nitric oxide bioavailability, and immune cells. For example, previous studies suggested that mRNA expression of renal α2B-adrenergic receptor in male spontaneously hypertensive rats is two times higher compared with females, which could contribute to higher blood pressure levels in males. In addition, males have greater expression of classical RAS components (mainly constrictor) than females, while non-classical RAS (mainly dilator) is enhanced in females.
Our study found that the metabolic risk factors of cognitive function differed from male to female patients. In male patients, hyperglycemia was associated with a worse immediate memory index score. Dyslipidemia was associated with worse language, attention, delayed memory index scores, and total score in female patients. The multivariate analyses further demonstrated that there are independent effects of hyperglycemia in males and dyslipidemia in females on cognitive ability. Zhuo et al. [40] also found that dyslipidemia is a risk factor for cognitive function in female patients with schizophrenia. A few studies have examined associations between metabolic risk factors and neurocognitive function in schizophrenia by sex. The study by Bosia et al. [41] showed that MetS was only closely related to executive function in female patients with schizophrenia. One study indicated that BMI was only correlated with male patients’ cognitive functions, including language, visuospatial skill, and attention [27]. Although not consistent with our findings, these studies demonstrate the association between metabolic risk factors and cognitive function in schizophrenia may be sex-specific. Some factors may contribute to the sex-specific association between metabolic abnormalities and cognitive function in schizophrenia. The following are the possible explanations.
Firstly, patients included in our study have a diverse history of antipsychotic treatment. Some studies have reported the effects of antipsychotic medications on cognitive function [42]. Metabolic abnormalities induced by antipsychotic drugs have also been widely reported in previous studies [43]. On the other hand, studies demonstrated the sex differences in antipsychotic treatment [44,45]. Almost all antipsychotic meditations work through the dopaminergic blockade, and the dopaminergic system is sexually dimorphic [46]. Although we compared the type of antipsychotic medication currently used between male and female patients, and there is no significant difference, it is difficult for us to evaluate the influence of antipsychotic medication previously used. Therefore, antipsychotic drug use may be one of the reasons that contribute to sex-differentiated associations of metabolic abnormalities with cognitive function in schizophrenia.
Secondly, sex hormones may also contribute to the sex-specific association between metabolic risk factors and cognitive function in schizophrenia. Sex steroid hormones are significantly associated with metabolism regulation [47]. Studies in mice have shown that estrogen depletion results in excess body fat and insulin resistance, and estrogen replacement treatment can protect estrogen-deficient mice from metabolic disease. The menopause transition induces a series of metabolic disturbances, such as obesity, glucose intolerance, and increased appetite [48,49]. On the other hand, it is reported that estrogen benefits cognitive function. Researchers found that estrogen supplementation in mice significantly enhanced their performances in cognitive tests, such as reinforcement alternation in the T-maze and working memory performance in the eightarm radial maze [50,51]. Women experience a range of cognitive changes during perimenopause, including reduced processing speed and verbal memory [52]. Atherosclerosis is one of the main mechanisms that metabolic disorders cause cognitive impairment [4]. It is reported that sex hormones are involved in the process of atherosclerosis. Estrogens and testosterones are proven to benefit lipid metabolism and have an anti-inflammatory effect, such as decreasing plaque formation and repressing the expression of tumor necrosis factor α, interleukin (IL)-1, and IL-6,53 which could slow down the process of atherosclerosis. In summary, sex-specific associations between metabolic risk factors and cognitive function in schizophrenia may be related to the hormonal status of patients. However, the underlying mechanisms of sex-specific effects of certain metabolic risk factors on the specific domain of cognitive functions need further investigation in the future.
There were some limitations to our research. Firstly, our study is a cross-sectional study, so the cause-effect relationship between metabolic disorders and cognitive performances in schizophrenia needs to be investigated further in prospective studies. Secondly, additional studies on the effects of sex hormones, such as estrogen, testosterone, and progesterone, on metabolism and cognitive function may help deepen our understanding of the mechanism involved. In addition, we did not have a drug-naïve group, which may make us more cautious when interpreting the results.
Taken together, our study suggests that sex should be considered when evaluating the impact of metabolic disorders on cognitive function in schizophrenia patients. This consideration may help to provide more precise preventative and treatment strategies for the management of cognitive deficits. Few studies take sex into account when exploring the association of metabolic disorders and cognitive deficits in schizophrenia. Our study provides some clues for further investigation in a larger cohort.