INTRODUCTION
Prolonged social withdrawal (hikikomori) is a phenomenon characterized by the avoidance of social interactions for more than half a year [1]. This kind of social withdrawal has attracted the attention of psychologists and other medical professionals in Japan, and similar cases have recently been reported in countries such as Australia, France, Italy, South Korea, Spain, and the USA [2-4]. An epidemiological study of hikikomori in a community-based population aged 20 to 49 years in Japan revealed that 1.2% had experienced the phenomenon in their lifetime [5], and a cross-sectional telephone-based survey in Hong Kong revealed that 1.9% of those aged 12 to 29 years had these experiences as well [6].
Most individuals undergoing long-term social withdrawal face health difficulties in their lives. For example, they have a significantly lower quality of life than those who have never experienced it [7], and show deterioration in physical health, including nutritional disorders and voice disturbances [8], obesity, and elevated blood pressure [9]. Kondo et al. [10] showed that 80.3% of individuals with hikikomori who utilized public mental health welfare services were diagnosed with some form of psychiatric disorder(s), including 33.3% who needed pharmacotherapy for conditions such as schizophrenia, mood disorders, or anxiety disorders, and that only one individual did not meet any DSMIV-TR diagnostic criteria. Furthermore, the ambivalent attachment style is associated with hikikomori [11]. Previous studies have reported that the main characteristics of people in long-term withdrawal are restricted social activity [12,13] and associated psychological, social, and behavioral effects [14]. Thus, most previous psychological studies have concentrated on clarifying the psychological, social, and behavioral characteristics of individuals with hikikomori [4,15] and identifying risks [16], but little has been identified in relation to an intervention target for hikikomori.
It is presumed that psychological stress is one of the factors responsible for hikikomori [17]. It could be argued that individuals use social withdrawal as a strategy for reducing psychological stress by avoiding social activities, but hikikomori is not necessarily reduced even when psychological stress is reduced. Therefore, there should be factors other than psychological stress that influence hikikomori, and identifying these factors can lead to the development of effective interventions for hikikomori. According to the psychological stress model [18], we can assume a process in which hikikomori is sustained by functioning as prolonged stress coping. In other words, it is plausible to investigate stress coping as a factor that influences hikikomori.
In addition, previous research reported people with hikikomori have low psychological flexibility [19]. Psychological flexibility is described as the “ability to contact the present moment more fully as a conscious human being, and to change or persist in behavior when doing so serves valued ends.” [20] One can assume that psychological inflexibility influences hikikomori as experiential avoidance, which is one concepts that is characteristic of psychological inflexibility, and is also related to psychological distress and maladaptive behavior [21].
Self-compassion may also be associated with hikikomori, because self-compassion is associated with loneliness [22] and loneliness is one of the factors associated with social withdrawal [23]. Neff [24] describes self-compassion as follows:
Being touched by and open to one’s own suffering, not avoiding or disconnecting from it, generating the desire to alleviate one’s suffering and to heal oneself with kindness. Self-compassion also involves facilitating nonjudgmental understanding to one’s pain, inadequacies and failures, so that one’s experience is seen as part of the larger human experience [24].
Self-compassion is negatively associated with depression, anxiety [25], and homesickness [26], and positively associated with well-being [27].
The current exploratory study investigates the effects of psychological stress, self-compassion, psychological inflexibility, and stress coping on hikikomori behaviors. Furthermore, this study examines the factors that change hikikomori by comparing the effects on hikikomori behaviors between people with hikikomori and people who have no experience of hikikomori. Clarifying these associations could be crucial for identifying intervention targets.
METHODS
Participants
Data were collected by recruiting participants from a large-scale web-based sample managed by a major, nationwide Internet research corporation, Rakuten Insight, Inc. (Tokyo, Japan), which maintains a pool of 2.2 million members in Japan. The sample consisted of 200 individuals who were asked whether they met the criteria for prolonged social withdrawal (hikikomori) [1]. First, we screened participants by asking 1) whether they had the experience of meeting the presented definition of hikikomori and 2) if they had the experience, how long it had lasted. If they answered that they had met the definition of hikikomori and that the duration was 6 months or more, they were classified into the hikikomori group. Recruitment was completed when each group had 100 people. Participants were classified into two groups: individuals with no experience of hikikomori (control group) and those who have experienced hikikomori (hikikomori group). To be eligible for the study, participants had to respond to all items. All participants voluntarily agreed to take part in the study, and were free to withdraw at any time. The age range of the participants was 23-49 years, the range of hikikomori duration in the hikikomori group was 6-304 months, the range of the number of days going out per month was 0-31 for the hikikomori group, and 4-31 for the control group (Table 1). Difficulty in social participation was scored on a 10-point scale ranging from 1 (“never experience difficulty”) to 10 (“certainly experience difficulty”), with the hikikomori group obtaining a mean score of 6.13 (SD=2.78), and the control group obtaining a mean score of 3.32 (SD= 2.34). There was a significant difference between the groups in difficulty in social participation [t(192.37)=7.73, p<0.001, d=1.09]. Residences were distributed between the following regions: Hokkaido (8.0%), Tohoku (5.5%), Kanto (40.0%), Chubu (14.5%), Kinki (14.5%), Chugoku (5.0%), Shikoku (3.0%), and Kyushu (9.5%).
Instruments
Demographics
Participants reported their age, sex, and experience of hikikomori in the present or the past, and the duration of their experience.
Adaptive Behaviors Scale for Hikikomori (ABS-H)
We used the self-report version of the Adaptive Behaviors Scale for Hikikomori (ABS-H) [12,28] to evaluate hikikomori behaviors. The ABS-H comprises 26 items to assess the level of social interaction for individuals with hikikomori. It includes four subscales: interaction (social interaction with others), family (social interaction with family members), values (behaviors that match the values of individuals with hikikomori), and social participation (going to school or work) [12,28]. A higher score indicated less frequent hikikomori behaviors. Participants rated the frequency of their social interaction on a 4-point Likert scale, ranging from 0 (“rarely”) to 3 (“often”). The ABS-H achieved adequate reliability, as well as criterion-related, discriminant, and construct validity [12]. Cronbach’s alpha coefficient for the total scale was 0.94, and each subscale ranged from 0.76 to 0.92 in this study.
Japanese version of the Self-Compassion Scale Short Form (SCS-J-SF)
We used the Japanese version of the Self-Compassion Scale Short Form (SCS-SF) [29-32] to evaluate self-compassion. The SCS-J-SF comprises 12 items and involves two factors. Positive factors include self-kindness, common humanity, and mindfulness; negative factors include self-judgment, isolation, and over-identification [33]. Participants rated the frequency of their self-compassion on a 5-point Likert scale ranging from 1 (“almost never”) to 5 (“almost always”). The SCS-J-SF has adequate reliability and construct validity [30]. Cronbach’s alpha coefficient was 0.80 in this study.
Japanese version of the Acceptance and Action Questionnaire-II (AAQ-II)
We used the Japanese version of the Acceptance and Action Questionnaire (AAQ-II) [34,35] to evaluate psychological inflexibility. The AAQ-II comprises seven items and one factor [34]. Participants rated experienced avoidance on a 7-point Likert scale ranging from 1 (“never true”) to 7 (“almost always true”). Higher scores indicated greater levels of psychological inflexibility. The AAQ-II has adequate reliability and discriminant and convergent validity [34]. Cronbach’s alpha coefficient was 0.93 in this study.
Japanese version of the Brief Coping Orientation to Problems Experienced (COPE) inventory
We used the Japanese version of the Brief COPE inventory to evaluate stress coping [36-38]. The Brief COPE comprises 28 items involving 14 factors: self-distraction, active coping, denial, substance use, using emotional support, using instrumental support, behavioral disengagement, venting, positive reframing, planning, humor, acceptance, religion, and self-blame [36,38]. Participants rated stress coping on a 4-point Likert scale ranging from 1 (“I usually don’t do this at all”) to 4 (“I usually do this a lot”). Higher scores indicated greater levels of coping skills. Previous studies reported the reliability and validity of the Brief COPE [36,38]. Cronbach’s alpha coefficient for each subscale ranged from 0.61 to 0.92; however, it was low for the self-distraction subscale (0.49) in this study. The low coefficient for the self-distraction subscale was consistent with a previous study (0.46) [38].
Stress Response Scale-18 (SRS-18)
We used the Stress Response Scale (SRS-18) to evaluate psychological stress [39]. The SRS-18 has 18 items involving three factors: depression-anxiety, irritability-anger, and helplessness [39]. Participants rated stress response on a 4-point Likert scale ranging from 0 (“never true”) to 3 (“almost always true”). Higher scores indicated greater levels of stress response. The SRS-18 has adequate reliability and content and discriminant validity [39]. Cronbach’s alpha coefficient was 0.96 in this study.
Data analysis
Data were analyzed using R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria) [40]. We calculated the means, standard deviations, and correlation coefficients between hikikomori behavior and the other variables. We performed hierarchical multiple regression analyses wherein sex, age, and group (hikikomori or control group) were added in step 1 as control values, and psychological stress, self-compassion, psychological inflexibility, and stress coping were added in step 2. The interaction terms were added in step 3 to examine the differences between groups. As a result of the correlation analyses, variables showing medium or large correlation coefficients (r>0.40) with hikikomori behaviors were inserted into the hierarchical multiple regression model.
Ethical considerations
The study was approved by the local research ethics committee of the institute to which the author belongs (Approval number 90). We obtained participants’ informed consent before conducting the study. In consideration of individuals’ privacy, the study was carried out anonymously. Participants were informed that submission of their responses would be regarded as consent.
RESULTS
Table 1 shows the demographic characteristics and Table 2 shows the mean values, standard deviations, and effect sizes of hikikomori behavior, psychological stress, self-compassion, stress coping, and psychological inflexibility scores. The number of days going out was significantly higher in the control group than in the hikikomori group (t=5.09, p<0.001).
Pearson’s correlation coefficient was significant between hikikomori behavior and psychological stress, self-compassion, psychological inflexibility, and stress coping scores (Supplementary Table 1 in the online-only Data Supplement). Variables (active coping and use of instrumental support, behavioral disengagement, planning stress coping, self-compassion, psychological stress, psychological inflexibility) showing a medium or large size correlation coefficient (r>0.40) for hikikomori behavior were selected as parameters.
The adjusted coefficient of determination in the hierarchical multiple regression analyses was significant in step 1 (R2 adj=0.24, p<0.001), and the ΔR2 in step 2 was significant (ΔR2=0.32, p<0.001). Use of instrumental support stress coping (B=0.24, p<0.001) and self-compassion (B=0.19, p=0.01) indicated a positively significant standardized partial regression coefficient, whereas behavioral disengagement stress coping (B=-0.14, p=0.02) and psychological stress (B=-0.20, p=0.003) indicated an inverse relationship (Table 3). Psychological inflexibility, active coping, and planning coping indicated no significance.
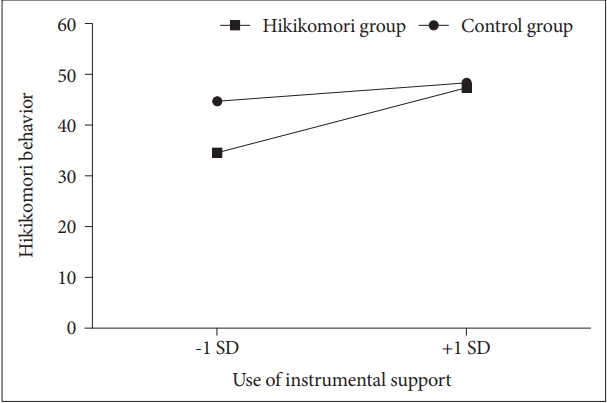
The ΔR2 in step 3 was significant (ΔR2=0.03, p=0.04) and demonstrated significant interaction effects between groups (hikikomori or control group) and use of instrumental support (Figure 1). Simple slope analysis showed that the use of instrumental support was significant for hikikomori behaviors in the hikikomori group (hikikomori group: B=0.40, p< 0.001; control group: B=0.11, p=0.16). The variance inflation factor (VIF) did not indicate a problem of multicollinearity (VIFs<3.20).
DISCUSSION
This exploratory study investigated the effects of psychological stress, self-compassion, psychological inflexibility, and stress coping on hikikomori behaviors. It also studied the differences in the effects of psychological factors on hikikomori between people with hikikomori and people with no experience with hikikomori. The results showed that the use of instrumental support and behavioral disengagement stress coping, self-compassion, and psychological stress influenced hikikomori behaviors, but psychological inflexibility and some stress coping skills did not influence the same. Furthermore, instrumental support levels were associated with lower hikikomori behaviors in the hikikomori group, but not in the control group.
Influence of psychological stress, self-compassion, psychological inflexibility, and stress coping on hikikomori behaviors
The results suggested that the use of instrumental support and behavioral disengagement stress coping skills, self-compassion, and psychological stress influenced hikikomori; therefore, therapy targeting these factors may help improve hikikomori. As hikikomori is often triggered by high-stress events, interventions to reduce psychological stress have been used for early hikikomori tendencies [1]. The results indicate that is it necessary to assess not only psychological stress but also stress coping skills (support seeking or disengagement coping) and self-compassion when clinicians choose a psychological approach. Further studies are needed to determine whether interventions that focus on self-compassion can, in fact, relieve hikikomori characteristics as this finding suggests. Previous findings have shown that self-compassion can play a mediating role between psychosocial factors. For instance, Terry et al. [26] showed that self-compassion negatively mediated the relationship between satisfaction with social life and homesickness, and Zhang et al. [41] showed that self-compassion negatively mediated the relationship between stressful experiences and negative affect. The findings of this study support those of previous studies. Compassion-based interventions are one approach to reducing psychological distress and improving well-being by increasing self-compassion [42]. This intervention may be effective in improving hikikomori, because these individuals often have high chronic psychological stress.
Psychological inflexibility, active coping, and planning coping did not influence hikikomori. Based on the fact that all of these variables showed a medium-sized or larger correlation with hikikomori, it is possible that the relationship with psychological inflexibility or stress coping skills and hikikomori are spurious correlations.
Results for the hikikomori group showed that higher hikikomori behaviors were present in individuals with low use of instrumental support than in people with high use of instrumental support. Kondo et al. [10] found that non-help-seeking hikikomori people had lower Global Assessment of Functioning (GAF) scores than those who engaged in treatment. The result of this study support this finding because “use of instrumental support” includes support-seeking coping. Psychosocial support will be needed depending on the characteristics of the case. More specifically, in the case of low support seeking, the first step will be family support [43,44], home visiting support [45,46], or an Internetbased approach to increase support seeking, and the next step will be therapy focused on psychological stress and self-compassion for the person with hikikomori. It may be also useful to include the findings of this study in the knowledge that families should acquire. In addition, it may help prevent the reduction of self-compassion in people with hikikomori by telling their families, for example, not to blame them for being in a state of hikikomori.
Limitations
Although the study could identify the factors that influence hikikomori, it also has some limitations. First, although the average duration of hikikomori among participants in this study was about three and a half years, recent epidemiological studies have indicated that long-term hikikomori cases are the most frequent. For example, 34.7% of those aged between 15 and 39 years [47] and 46.7% aged between 40 and 64 years [48] had been socially withdrawn for more than seven years. Therefore, further studies are needed to clarify whether the findings of this study can be generalized to longer-term cases and whether the difference in the length is due to the recruitment method. In addition, the potential limited representativeness of a web-based sample also limits this study. To be sure, many people with hikikomori avoid others, including researchers and clinicians, so web-based research has the benefit of increasing access. However, it will be necessary to determine if the web-based sample is biased as the hikikomori sample.
This study is a cross-sectional study and no causal relationship has been identified. In this study, we examined the effects of psycho-behavioral factors on hikikomori to clarify the target of intervention in treating the condition, but it is quite possible that these factors interact with each other. Therefore, further follow-up and intervention studies may be needed to identify causal relationships. Previous studies reported that AAQ-II has poor construct validity as a measure of experiential avoidance [49]; therefore, the findings of this study should be interpreted with caution.
Further studies are also needed to clarify whether the findings are the same in cultures other than Japan, since it is known that there are cultural differences in self-compassion; self-compassion has been found to be lower in Japan than in the United States and Thailand [29,50]. Furthermore, the characteristics of hikikomori behavior may also be influenced by cultural differences [51]. For example, investigating the effects of differences in family relationships, work styles, and gender roles on the findings of this study could help develop a type-specific approach to intervene with hikikomori characteristics.
The hikikomori group had more men than women, which is consistent with many previous studies [5,10]. However, the proportion of women in the control group was higher than in the hikikomori group. This gender-ratio difference may have influenced the results.
In conclusion, this study suggests that not only psychological stress but also behavioral disengagement stress coping are positively associated with hikikomori behaviors, while instrumental support stress coping and self-compassion are negatively associated with these behaviors. Psychological inflexibility and the others stress coping skills do not directly associate with hikikomori behaviors. Assessing not only psychological stress but also instrumental support stress coping, including support seeking, will help hikikomori improve. In the future, it will be necessary to clarify effective support including family support, home visitation, or an Internet-based approach according to the characteristics of support seeking and self-compassion in people with hikikomori.