INTRODUCTION
Patients with obsessive-compulsive disorder (OCD) suffer from recurrent obsessions and compulsions that cause marked distress or impaired functioning. The Yale-Brown Obsessive Compulsive Scale (Y-BOCS) is the most widely used instrument for assessing these symptoms.1,2 The full version of the Y-BOCS is administered by a well-trained clinician during an interview that takes about 30 minutes. As the clinician-administered version can be time-consuming, a self-report version of the Y-BOCS was developed by Baer in 1991.3 Previous studies have compared the clinician-administered Y-BOCS with the self-report version4,5 and found significant correlations between individual items on the two scales (r=0.41 to 0.76) among 36 OCD patients.4 A more recent study with a larger sample also found that the total Y-BOCS scores on the two scales showed significant intraclass correlations (ICCs) (ICC=0.64) in 86 patients with OCD.5 They also found that the mean score on the clinician-administered Y-BOCS was significantly higher than that on the self-report version of the Y-BOCS.
However, no previous study has elucidated the factors related to discrepancies between the two versions of this instrument. In the assessment of depression, discrepancies between scores on the clinician-rated Hamilton Depression Rating Scale and the self-report Beck Depression Inventory have been associated with high neuroticism and low extraversion on the NEO-Five-Factor Inventory, a personality inventory.6 Although many studies have explored comorbid axis II personality disorders in OCD patients,7-10 no previous research has investigated the personality traits related to discrepancies between self-reported and clinician-administered measures of obsessive-compulsive symptoms. Despite variations in results regarding comorbid personality disorders, it is well known that patients with OCD have high rates of comorbidity with cluster-C personality disorders. Additionally, some studies have found that comorbid cluster-B personality disorders are associated with poor treatment response.11,12 Nonetheless, no previous study has examined relationships between personality traits and discrepancies between self-reports and clinician ratings. This study examined consistencies and discrepancies between the two versions of the Y-BOCS and elucidated the personality traits that affect such discrepancies.
METHODS
Participants
Patients were recruited from the OCD outpatient clinic at Seoul National University Hospital (SNUH) during 2006-2011. A total of 106 patients met DSM-IV criteria for obsessive-compulsive disorder (OCD).
None of the participants was taking medicine at intake; 48 patients were drug naive, and 58 had been unmedicated for at least 4 weeks. No patient had previously received cognitive-behavioral therapy. The sample consisted of 64 males and 42 females, with a mean age of 26.75┬▒8.31 years. The mean age of onset and the mean duration of illness were 19.33┬▒7.91 and 7.44┬▒6.50 years, respectively. The mean duration of participants' education was 14.23┬▒2.53 years. Participants suffered from the following comorbid axis I psychiatric disorders: mood disorder (n=22), general anxiety disorder (n=4), tic disorder (n=2), impulse-control disorder (n=1), and somatoform disorder (n=1). Participants who were diagnosed with schizophrenia or mental retardation were excluded. Participants with a history of significant neurologic or medical illness were also excluded. This study was approved by the Institutional Review Board of SNUH.
Clinical measures
Yale-Brown Obsessive Compulsive Scale (Y-BOCS)
We used the Yale-Brown Obsessive Compulsive Scale (Y-BOCS) to assess the severity of obsessions and compulsions. Symptom severity was measured in five domains: time spent, interference, distress, efforts to resist, and perceived control. Each domain was rated on a five-point Likert scale from 0 (not at all/none) to 4 (extreme).
All participants were assessed with the clinician-administered and self-report versions of the Y-BOCS.13 The clinician-administered Y-BOCS was administered by psychiatrists who worked at the OCD outpatient clinic at SNUH during 2006-2011. However, the therapist for the subjects did not participate in the Y-BOCS rating. Although we did not assess interrater reliability, all raters were clinically well-trained boardcertified psychiatrists who had sufficient experience with the Y-BOCS. Most patients (90.6%) were assessed with the clinician-administered Y-BOCS prior to completing the self-report Y-BOCS. Only 9.4% of the patients completed the selfreport version of the Y-BOCS first. The mean time between completion of the two versions of the Y-BOCS was 8.0 days.
Structured Clinical Interview for DSM-IV Axis II Disorders Personality Questionnaire (SCID-II-PQ)
Personality traits were assessed with the Korean version of the SCID-II-PQ, which consists of 119 items rated on a dichotomous (yes/no) scale.14 This study used the SCID-II-PQ as a screening tool given the high level of agreement (kappa=0.78) between the SCID-II clinical interview and the SCID-II personality questionnaire after adjusting the cut-off value.15
Statistical analysis
To investigate consistencies and discrepancies between scores on the two versions of the Y-BOCS, we used independent t-tests between means and calculated the intraclass correlation coefficients (ICCs) for the correlation analyses. We calculated discrepancy scores by subtracting the scores on the clinician-administered Y-BOCS from those on the self-report Y-BOCS.6 Multiple linear regression analysis was conducted to investigate whether personality traits were associated with discrepancies. Statistical analyses were performed using Predictive Analytics Software (PASW) version 18.0 (SPSS, Inc., Chicago, USA).
RESULTS
Consistencies and discrepancies between scores on clinician-administered and self-report versions of the Y-BOCS
The mean scores on the clinician-administered and self-report versions of the Y-BOCS are shown in Table 1. Independent t-tests revealed that scores on the clinician-administered Y-BOCS and on the obsession subscale were significantly higher than were those on the self-report versions. However, the difference between scores on the two versions of the compulsion subscale was not significant (p=0.372).
To assess the strength of the correlations, we calculated the ICC between the two versions of the Y-BOCS. We found significant correlations between scores on the two versions of the Y-BOCS and the obsession and compulsion subscales. However, a lower ICC was found for the obsession subscale (ICC=0.61, p<0.0001) than for the total Y-BOCS (ICC=0.70, p<0.0001) and the compulsion subscale (ICC=0.68, p<0.0001).
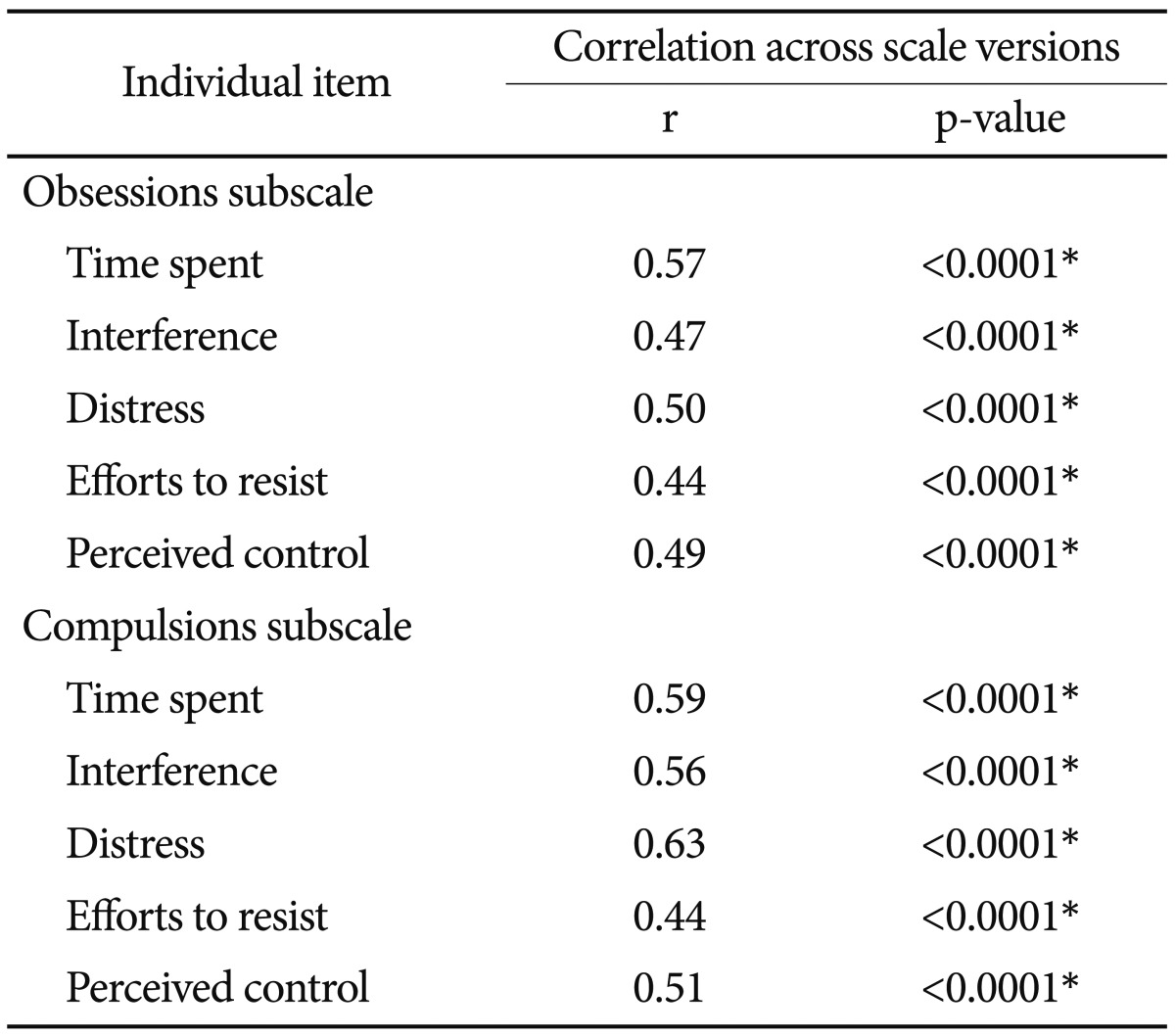
Table 2 presents the correlations between the scores on the individual items in the two versions of the Y-BOCS. Although significant correlations between scores on individual items were found, the correlations between the two versions of items addressing "efforts to resist obsessions" and "efforts to resist compulsions" were lower than were others (r=0.44 for item 4 on the obsession subscale, r=0.44 for item 9 on the compulsion subscale).
The internal consistency was high for both versions of the Y-BOCS. The Cronbach's alphas for the self-report Y-BOCS were 0.88 (total), 0.78 (obsession subscale), and 0.85 (compulsion subscale). Those for the clinician-administered Y-BOCS were 0.84 (total), 0.68 (obsession subscale), and 0.88 (compulsion subscale).
Total Y-BOCS scores can be classified into five groups according to severity: subclinical (0-7), mild (8-15), moderate (16-23), severe (24-31), and extreme (32-40). To assess the degree of consistency in this categorical classification, we calculated the value of the weighted kappa and found a moderate degree of agreement between the two scales (weighted kappa=0.43).
Relationships between Y-BOCS and SCID-II-PQ scores
We also investigated the relationship between symptom severity on the Y-BOCS and personality traits. The data indicated that the most common comorbid personality traits were obsessive-compulsive (71.70%), borderline (60.38%), narcissistic (55.66%), and avoidant (51.89%) (Table 3).
In addition, we examined correlations between SCID-II personality questionnaire scores and two versions of Y-BOCS scores (total scores, compulsion subscale scores and obsession subscale scores) (Table 4). The significant positive correlations were observed in cluster A and cluster C personality traits with the self-reported total Y-BOCS scores (r=0.27, p<0.01 for avoidant trait, r=0.25 for paranoid trait, p<0.05). This suggests that the obsessive-compulsive symptom severity is correlated with these personality traits. However, there were no significant correlations between the cluster B personality traits and the Y-BOCS scores.
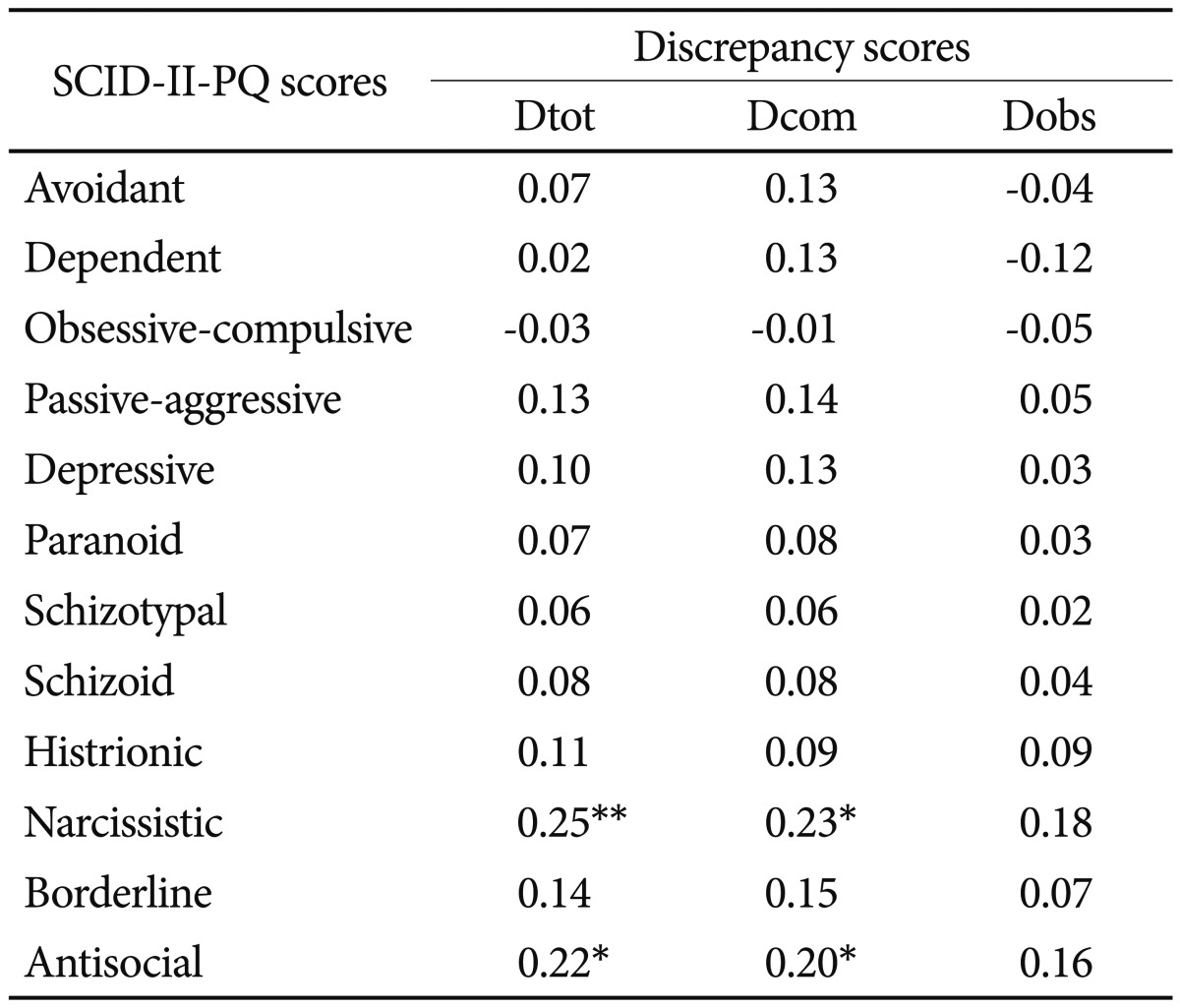
To elucidate the relationship of discrepancies between the self-report and clinician-administered scores with personality traits, we calculated discrepancy scores by subtracting clinician-administered Y-BOCS scores from self-report Y-BOCS scores (Table 5); thus, higher discrepancy scores reflected higher scores on the self-report than on the clinician-administered Y-BOCS, indicating that patients rated their symptoms as more severe than did clinicians. Table 5 shows that the discrepancies between total Y-BOCS scores (Dtot) were positively correlated with narcissistic (r=0.25, p<0.01) and antisocial (r=0.22, p<0.05) personality traits. Furthermore, discrepancies on the compulsion subscale (Dcom) were also positively correlated the narcissistic (r=0.23, p<0.05) and antisocial (r=0.20, p<0.05) personality traits. However, we found no significant correlations between scores on the personality questionnaire and discrepancies between the two scores on the obsession subscale (Dobs). To exclude the effect of axis I comorbid conditions, such as depressive and other anxiety disorders, we conducted an additional analysis among OCD patients without comorbid axis I disorders (n=80). Comparisons of the mean scores on the Y-BOCS and the discrepancy scores for all patients with OCD (n=106) with that for patients without any axis I comorbid disorders (n=80) revealed no significant differences between the two groups. We also observed significant positive correlations between narcissistic personality traits and discrepancies in total Y-BOCS (r=0.27, p=.014) and compulsion subscale (r=0.23, p=0.044) scores in patients with OCD but without comorbid conditions (n=80). However, we found no significant positive correlations between antisocial personality traits and discrepancies between the scores on the two versions of the Y-BOCS when patients with OCD with axis I comorbid conditions were excluded, suggesting that the correlations between antisocial personality traits and discrepancy scores may have been influenced by the inclusion of patients with comorbid axis I disorders in our OCD sample.
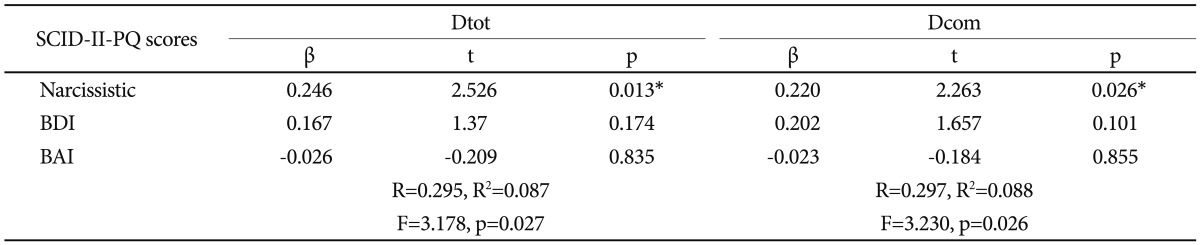
Furthermore, narcissistic personality traits had significant effects on the discrepancies between scores on the two versions of both the full Y-BOCS and the compulsion subscale when scores on the self-report BDI and BAI were controlled in multiple linear regression analysis (Table 6).
DISCUSSION
In this study, we found that mean scores on the clinician-administered Y-BOCS were significantly higher than were those on the self-report version. The main difference between the two versions of the Y-BOCS was attributable to the obsession subscale, which was the only subscale on which scores on the two versions differed significantly. This implies that clinicians tend to rate obsessive symptoms as more severe than do patients. The mean scores on the two compulsion subscales did not differ significantly. There was a previous report which found that scores on the clinician-rated Y-BOCS were higher than the self-rated scores.5 However, the significant differences were found between scores on the compulsion subscale not on the obsession subscale.5 These results can be interpreted in several ways. First, we believe that compulsions are easier to rate than are obsessions, which may be due to the characteristics of the two phenomena. Indeed, obsessions are more subjective and difficult to rate, whereas compulsions can be more objective and easier to rate, which may reduce discrepancies between the two compulsion scores. Furthermore, the ICCs for the obsession subscales (ICC=0.61) were lower than were those for the compulsion subscales (ICC=0.68), which also suggests a greater discrepancy between obsession than between the compulsion subscales.
With regard to the comparisons between individual items on the two versions of the Y-BOCS, the Pearson's correlation coefficients for all items ranged from r=0.44 to r=0.63 (p<0.0001) (Table 2). Items addressing "efforts to resist obsessions" (item 4) and "efforts to resist compulsions" (item 9) had the lowest value (r=0.44), which is consistent with the results of a previous study in which "efforts to resist obsessions" also had the lowest value (r=0.26).5 The mean scores of these items in the clinician-rated Y-BOCS (2.09┬▒1.23 for item 4 and 2.04┬▒ 1.23 for item 9) were higher than were those on the self-report version (1.61┬▒0.92 for item 4 and 1.79┬▒1.13 for item 9), suggesting that clinicians underestimate the efforts expended by patients to resist these symptoms.
Next, we investigated relationships between Y-BOCS scores and personality traits. According to our data, the most common comorbid personality traits in patients with OCD were obsessive-compulsive (71.70%), borderline (60.38%), narcissistic (55.66%), and avoidant (51.89%) (Table 3). It has been established that cluster-C personality traits are common in patients with OCD.7-9 It is noteworthy that the present study found that cluster-B personality traits (borderline and narcissistic traits) were common in patients with OCD. This result is consistent with those of a previous study, which found that OCD patients were more likely to have comorbid borderline personality disorder than were normal controls.18 Additionally, another study found that patients with OCD reported having 22% of the narcissistic and 14% of the borderline personality traits included in the SCID-II screening questionnaire.9
One of the common features of cluster-B personality disorders is impulsivity. Indeed, the diagnostic criteria for borderline personality disorder include impulsivity that is potentially self-damaging (e.g., substance abuse, reckless driving, binge eating). OCD is located at the compulsive end of the compulsive-impulsive spectrum, whereas borderline personality disorder is located at the impulsive end. Because compulsivity and impulsivity both involve repetitive behaviors and the inability to delay or inhibit these behaviors, there are substantial areas of overlap between OCD and borderline personality disorder.19 Additionally, both the compulsiveness in OCD and the impulsiveness in cluster-B personality traits involve an increase in tension before enactment of the repetitive behavior, which is followed by a relief of anxiety.20
Furthermore, we found that the discrepancy between selfreported and clinician-rated Y-BOCS scores were positively correlated with scores for narcissistic personality traits (Table 5). This implies that the suffering of patients with the narcissistic personality traits may be underestimated by clinicians. Additionally, we also found positive correlations between the discrepancy between the compulsion subscales (Dcom) and scores for narcissistic personality traits. These data suggest that subjective discomfort due to compulsive symptoms may be underestimated by clinicians when scores for narcissistic personality traits are high. The definition of narcissism includes increased interest in one's self.21 Thus, patients with OCD who have narcissistic personality traits may rate their symptoms to be more severe than do clinicians. Additionally, cluster-B personality traits have dramatic, emotional, or erratic qualities,21 which may result in a greater discrepancy in the two versions of the compulsion subscales. According to the regression analysis, narcissistic personality traits had a significant effect on discrepancies between scores on the two versions of the Y-BOCS and of the compulsion subscale. This finding suggests that, among the cluster B-personality traits, narcissistic traits are significantly associated with discrepancy scores.
As this research was an exploratory investigation of the possible relationship between Y-BOCS scores and personality traits, correlation analyses were conducted using an alpha value of 0.05 as the threshold for statistical significance. When Bonferroni corrections were performed for the correlation analysis between self-reported/clinician-administered Y-BOCS scores and personality traits, only the Pearson's correlation coefficient for the relationship between depressive traits and Sobs (r=0.31, p=0.001) and Cobs (r=0.31, p=0.001) remained significant (p<0.0028). Furthermore, the Pearson's correlation coefficients between discrepancy scores and narcissistic or antisocial traits were not significant after Bonferroni correction. However, these results may provide clues about potential predictors of the discrepancy scores in the multiple regression analysis.
The analysis of personality traits performed in this study was limited by the fact that no SCID-II clinical interviews were conducted. It has been reported that more patients are found to suffer from a personality disorder when the SCID-II screening questionnaire (73%) than when the SCID-II interview (54%) is used.14 However, when the threshold for diagnosis was adjusted, the rates approached identity: 58% and 54%, respectively.14 Thus, although the SCID-II personality questionnaire cannot itself determine whether patients have a personality disorder, it can nonetheless be a useful and convenient tool for screening personality traits in clinical settings.
This study found relatively higher frequencies of all types of personality traits than did previous studies.9,22 This may have resulted from the different clinical characteristics of participants in different studies. Additionally, one previous study found that patients with OCD no longer met criteria for a personality disorder after 4 months of treatment,23 suggesting that treatment may affect a comorbid personality disorder as well as the severity of OCD itself. Previous studies that found lower rates of each type of personality trait than did our study included medicated patients with OCD who were clinically improved.9 However, our study included patients with OCD who had no history of treatment for their life or at least one month at the time of assessment, suggesting that patients with more severe psychopathology may have been included in our sample. Thus, differences in the clinical characteristics of samples may have contributed to the different rates of comorbid personality disorder among studies.23
In conclusion, this is the first study to elucidate relationships between personality traits and discrepancies in self-reported and clinician-assessed ratings of obsessive-compulsive symptoms. Our investigation of the discrepancies between the two versions of Y-BOCS (clinician-administered and self-report) suggests that clinicians tend to rate obsessive symptoms as being more severe than do patients. However, clinicians may underestimate the subjective discomfort due to compulsive symptoms experienced by patients with narcissistic personality traits. Therefore, clinicians should consider the effect of personality traits on symptom severity in the treatment of OCD. Further research using SICD-II interviews to examine relationships between personality traits and Y-BOCS scores should be conducted in the future.